

Hyperglycemic hemianopia: A case report
- PMID: 33728317
- PMCID: PMC7942036
- DOI: 10.12998/wjcc.v9.i7.1720
Hyperglycemic hemianopia: A case report
Abstract
Background: Nonketotic hyperglycemia (NKH) is characterized by hyperglycemia with little or no ketoacidosis. Diverse neurological symptoms have been described in NKH patients, including choreoathetosis, hemiballismus, seizures, and coma in severe cases. Homonymous hemianopia, with or without occipital seizures, caused by hyperglycemia is less readily recognized.
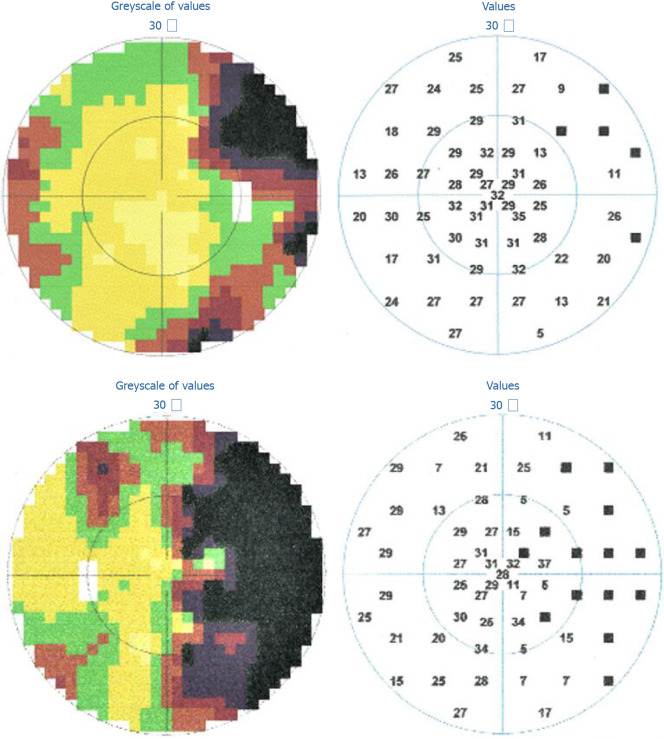
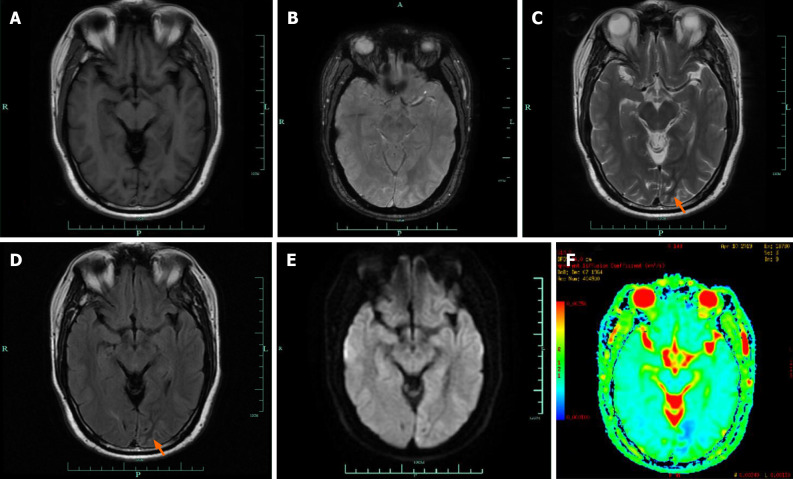
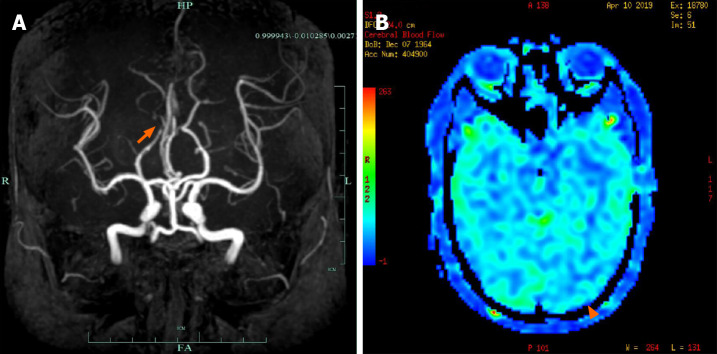
Case summary: We describe a 54-year-old man with NKH, who reported seeing round, colored flickering lights with right homonymous hemianopia. Cranial magnetic resonance imaging demonstrated abnormalities in the left occipital lobe, with decreased T2 signal of the white matter, restricted diffusion, and corresponding low signal intensity in the apparent diffusion coefficient map. He responded to rehydration and a low-dose insulin regimen, with improvements of his visual field defect.
Conclusion: Patients with NKH may present focal neurologic signs. Hyperglycemia should be taken into consideration when making an etiologic diagnosis of homonymous hemianopia.
Keywords: Case report; Homonymous hemianopia; Imaging manifestations; Nonketotic hyperglycemia; Occipital seizures.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no competing interests.
Figures
References
-
- Bacanu G, Anghelescu L, Mihailov E, Wilkomm I. [Hyperosmolar Diabetic Coma without Acidoketosis] Med Interna (Bucur) 1965;17:353–359. - PubMed
-
- Chung SJ, Lee JH, Lee SA, No YJ, Im JH, Lee MC. Co-occurrence of seizure and chorea in a patient with nonketotic hyperglycemia. Eur Neurol. 2005;54:230–232. - PubMed
-
- Singh BM, Strobos RJ. Epilepsia partialis continua associated with nonketotic hyperglycemia: clinical and biochemical profile of 21 patients. Ann Neurol. 1980;8:155–160. - PubMed
-
- Guisado R, Arieff AI. Neurologic manifestations of diabetic comas: correlation with biochemical alterations in the brain. Metabolism. 1975;24:665–679. - PubMed
-
- Maccario M. Neurological dysfunction associated with nonketotic hyperglycemia. Arch Neurol. 1968;19:525–534. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
