

Contrast-Enhanced Ultrasound (CEUS) in Non-Traumatic Abdominal Emergencies
- PMID: 33728394
- PMCID: PMC7954641
- DOI: 10.1055/a-1347-5875
Contrast-Enhanced Ultrasound (CEUS) in Non-Traumatic Abdominal Emergencies
Abstract
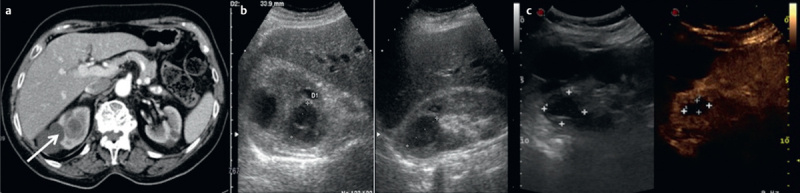
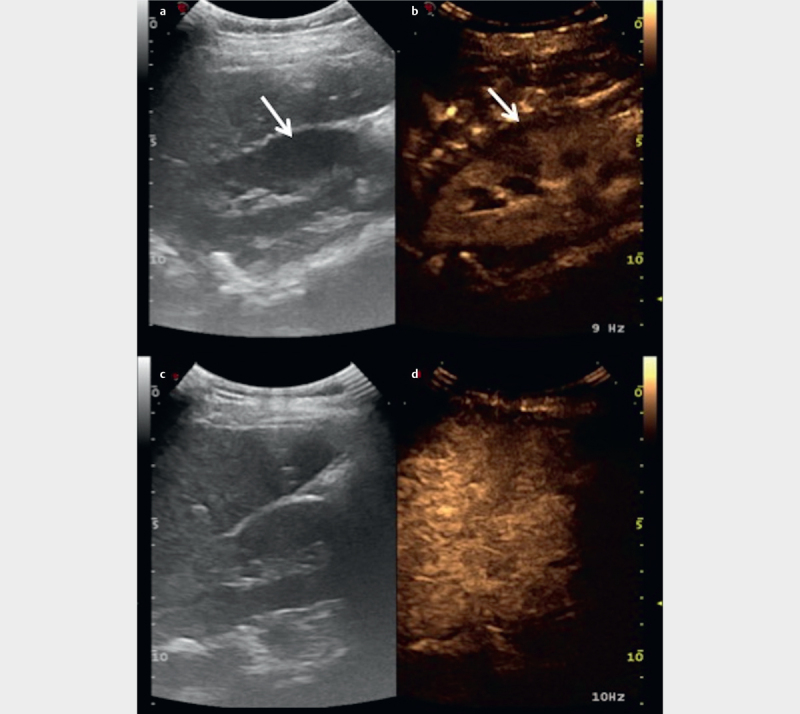
Conventional ultrasound imaging (US) is the first-line investigation in acute non-traumatic abdominal emergencies, but sometimes it needs further examinations, such as computed tomography (CT), to reach a certain diagnosis. Contrast-enhanced ultrasound (CEUS), through injection of contrast medium, may provide the radiologist with additional information that could not be investigated with baseline US. It could help reach a diagnosis and rapidly determine the proper therapy in an emergency setting. The purpose of this review is to explain and illustrate the various possibilities and limitations of CEUS in acute non-traumatic abdominal diseases, in particular acute inflammation, parenchymal infarcts, and hemorrhages.
Keywords: abdomen; acute; ultrasound; CT.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Conflict of Interest The authors declare that they have no conflict of interest related to the publication of this article.
Figures


References
-
- Stoker J, Van Randen A, Laméris W et al.Imaging patients with acute abdominal pain. Radiology. 2009;253:31–46. - PubMed
-
- Choe J, Wortman J R, Micheals A et al.Beyond appendicitis: Ultrasound findings of acute bowel pathology. Emerg Radiol. 2019;26:307–317. - PubMed
-
- Hunt D, Romero J. Contrast-enhanced ultrasound. Magn Reson Imaging Clin N Am. 2017;25:725–736. - PubMed
-
- Farina R, Catalano O, Stavolo C et al.Emergency radiology. Radiol Med. 2015;120:73–84. - PubMed
Publication types
LinkOut - more resources
Full Text Sources