

Visceral myopathy: clinical syndromes, genetics, pathophysiology, and fall of the cytoskeleton
- PMID: 33729000
- PMCID: PMC8285581
- DOI: 10.1152/ajpgi.00066.2021
Visceral myopathy: clinical syndromes, genetics, pathophysiology, and fall of the cytoskeleton
Abstract
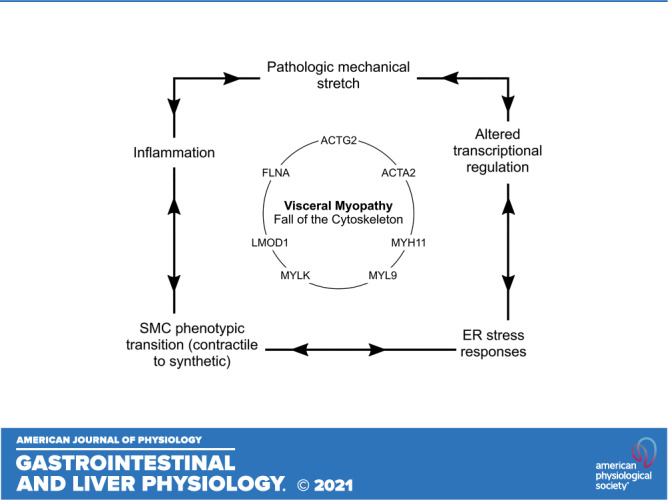
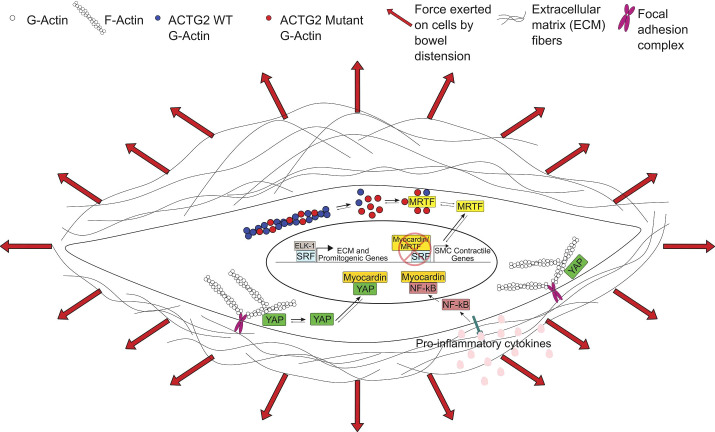
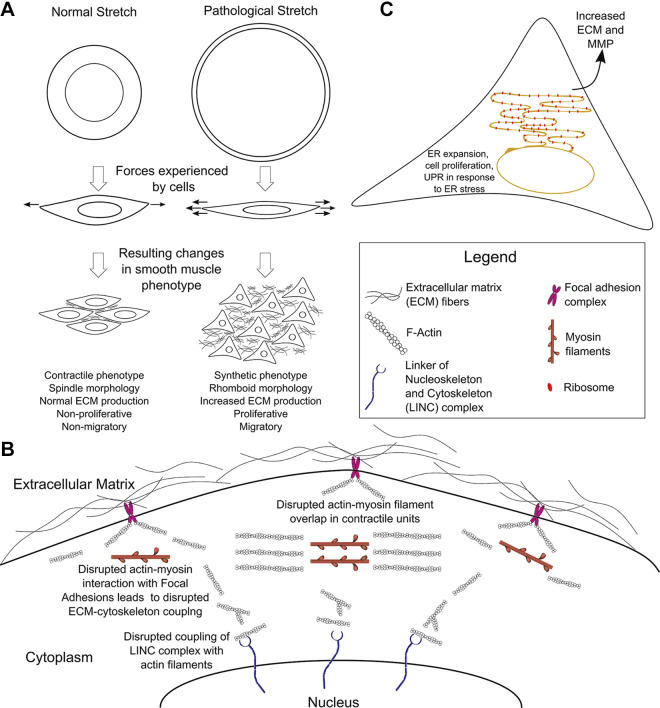
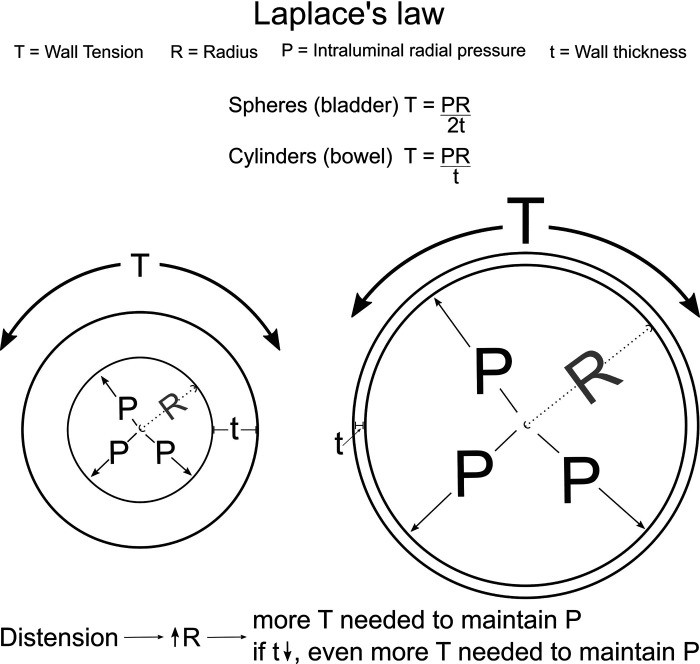
Visceral smooth muscle is a crucial component of the walls of hollow organs like the gut, bladder, and uterus. This specialized smooth muscle has unique properties that distinguish it from other muscle types and facilitate robust dilation and contraction. Visceral myopathies are diseases where severe visceral smooth muscle dysfunction prevents efficient movement of air and nutrients through the bowel, impairs bladder emptying, and affects normal uterine contraction and relaxation, particularly during pregnancy. Disease severity exists along a spectrum. The most debilitating defects cause highly dysfunctional bowel, reduced intrauterine colon growth (microcolon), and bladder-emptying defects requiring catheterization, a condition called megacystis-microcolon-intestinal hypoperistalsis syndrome (MMIHS). People with MMIHS often die early in childhood. When the bowel is the main organ affected and microcolon is absent, the condition is known as myopathic chronic intestinal pseudo-obstruction (CIPO). Visceral myopathies like MMIHS and myopathic CIPO are most commonly caused by mutations in contractile apparatus cytoskeletal proteins. Here, we review visceral myopathy-causing mutations and normal functions of these disease-associated proteins. We propose molecular, cellular, and tissue-level models that may explain clinical and histopathological features of visceral myopathy and hope these observations prompt new mechanistic studies.
Keywords: CIPO; MMIHS; cytoskeleton; visceral myopathy.
Conflict of interest statement
R. O. Heuckeroth is a consultant for BlueRock Therapeutics and served on a Scientific Advisory Panel for Takeda. None of the other authors has any conflicts of interest, financial or otherwise, to disclose.
Figures
References
-
- Thapar N, Saliakellis E, Benninga MA, Borrelli O, Curry J, Faure C, De GR, Gupte G, Knowles CH, Staiano A, Vandenplas Y, Di Lorenzo C. . Paediatric intestinal pseudo-obstruction: evidence and consensus-based recommendations from an ESPGHAN-Led Expert Group. J Pediatr Gastroenterol Nutr 66: 991–1019, 2018. doi: 10.1097/mpg.0000000000001982. - DOI - PubMed
-
- Vargas JH, Sachs P, Ament ME. Chronic intestinal pseudo-obstruction syndrome in pediatrics. Results of a national survey by members of the North American Society of Pediatric Gastroenterology and Nutrition. J Pediatr Gastroenterol Nutr 7: 323–332, 1988. doi: 10.1097/00005176-198805000-00003. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources