

Applying Latent Class Analysis on Cancer Registry Data to Identify and Compare Health Disparity Profiles in Colorectal Cancer Surgical Treatment Delay
- PMID: 33729186
- PMCID: PMC8435045
- DOI: 10.1097/PHH.0000000000001341
Applying Latent Class Analysis on Cancer Registry Data to Identify and Compare Health Disparity Profiles in Colorectal Cancer Surgical Treatment Delay
Abstract
Context: Colorectal cancer (CRC) surgical treatment delay (TD) has been associated with mortality and morbidity; however, disparities by TD profiles are unknown.
Objectives: This study aimed to identify CRC patient profiles of surgical TD while accounting for differences in sociodemographic, health insurance, and geographic characteristics.
Design: We used latent class analysis (LCA) on 2005-2015 Tennessee Cancer Registry data of CRC patients and observed indicators that included sex/gender, age at diagnosis, marital status (single/married/divorced/widowed), race (White/Black/other), health insurance type, and geographic residence (non-Appalachian/Appalachian).
Setting: The state of Tennessee in the United States that included both Appalachian and non-Appalachian counties.
Participants: Adult (18 years or older) CRC patients (N = 35 412) who were diagnosed and surgically treated for in situ (n = 1286) and malignant CRC (n = 34 126).
Main outcome measure: The distal outcome of TD was categorized as 30 days or less and more than 30 days from diagnosis to surgical treatment.
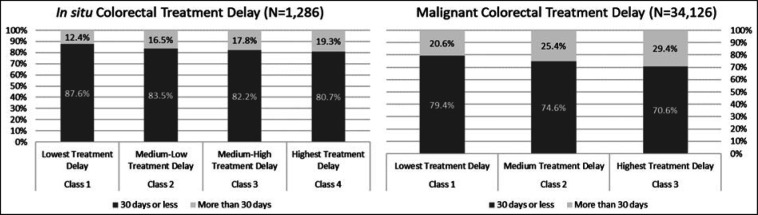
Results: Our LCA identified a 4-class solution and a 3-class solution for in situ and malignant profiles, respectively. The highest in situ CRC patient risk profile was female, White, aged 75 to 84 years, widowed, and used public health insurance when compared with respective profiles. The highest malignant CRC patient risk profile was male, Black, both single/never married and divorced/separated, resided in non-Appalachian county, and used public health insurance when compared with respective profiles. The highest risk profiles of in situ and malignant patients had a TD likelihood of 19.3% and 29.4%, respectively.
Conclusions: While our findings are not meant for diagnostic purposes, we found that Blacks had lower TD with in situ CRC. The opposite was found in the malignant profiles where Blacks had the highest TD. Although TD is not a definitive marker of survival, we observed that non-Appalachian underserved/underrepresented groups were overrepresented in the highest TD profiles. The observed disparities could be indicative of intervenable risk.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
A National Study of Colorectal Cancer Survivorship Disparities: A Latent Class Analysis Using SEER (Surveillance, Epidemiology, and End Results) Registries.Front Public Health. 2021 Feb 25;9:628022. doi: 10.3389/fpubh.2021.628022. eCollection 2021. Front Public Health. 2021. PMID: 33718323 Free PMC article.
-
Identifying Risk Profiles of Malignant Prostate Cancer Surgical Delay Using a Person-Centered Approach to Understand Prostate Cancer Disparities: The Constellation of Health Determinants Using Latent Class Analysis on Cancer Registry Data.Am J Mens Health. 2020 Nov-Dec;14(6):1557988320984282. doi: 10.1177/1557988320984282. Am J Mens Health. 2020. PMID: 33372564 Free PMC article.
-
Sociodemographic and Geographic Disparities of Prostate Cancer Treatment Delay in Tennessee: A Population-Based Study.Am J Mens Health. 2021 Nov-Dec;15(6):15579883211057990. doi: 10.1177/15579883211057990. Am J Mens Health. 2021. PMID: 34836465 Free PMC article.
-
Assessing health disparities in breast cancer incidence burden in Tennessee: geospatial analysis.BMC Womens Health. 2021 May 3;21(1):186. doi: 10.1186/s12905-021-01274-9. BMC Womens Health. 2021. PMID: 33941168 Free PMC article.
-
Disparities in localized malignant lung cancer surgical treatment: A population-based cancer registry analysis.Cancer Med. 2023 Mar;12(6):7427-7437. doi: 10.1002/cam4.5450. Epub 2022 Nov 17. Cancer Med. 2023. PMID: 36397278 Free PMC article.
Cited by
-
A National Study of Colorectal Cancer Survivorship Disparities: A Latent Class Analysis Using SEER (Surveillance, Epidemiology, and End Results) Registries.Front Public Health. 2021 Feb 25;9:628022. doi: 10.3389/fpubh.2021.628022. eCollection 2021. Front Public Health. 2021. PMID: 33718323 Free PMC article.
-
Treatment delay significantly increases mortality in colorectal cancer: a meta-analysis.Geroscience. 2025 Jun;47(3):5337-5353. doi: 10.1007/s11357-025-01648-z. Epub 2025 Apr 8. Geroscience. 2025. PMID: 40198462 Free PMC article.
References
-
- Siegel RL, Miller KD, Goding Sauer A, et al. Colorectal cancer statistics, 2020. CA Cancer J Clin. 2020;70(3):145–164. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
