

Association Between Anesthesiologist Volume and Short-term Outcomes in Complex Gastrointestinal Cancer Surgery
- PMID: 33729435
- PMCID: PMC7970385
- DOI: 10.1001/jamasurg.2021.0135
Association Between Anesthesiologist Volume and Short-term Outcomes in Complex Gastrointestinal Cancer Surgery
Abstract
Importance: Intraoperative anesthesiology care is crucial to high-quality surgical care. The clinical expertise and experience of anesthesiologists may decrease the risk of adverse outcomes.
Objective: To examine the association between anesthesiologist volume and short-term postoperative outcomes for complex gastrointestinal (GI) cancer surgery.
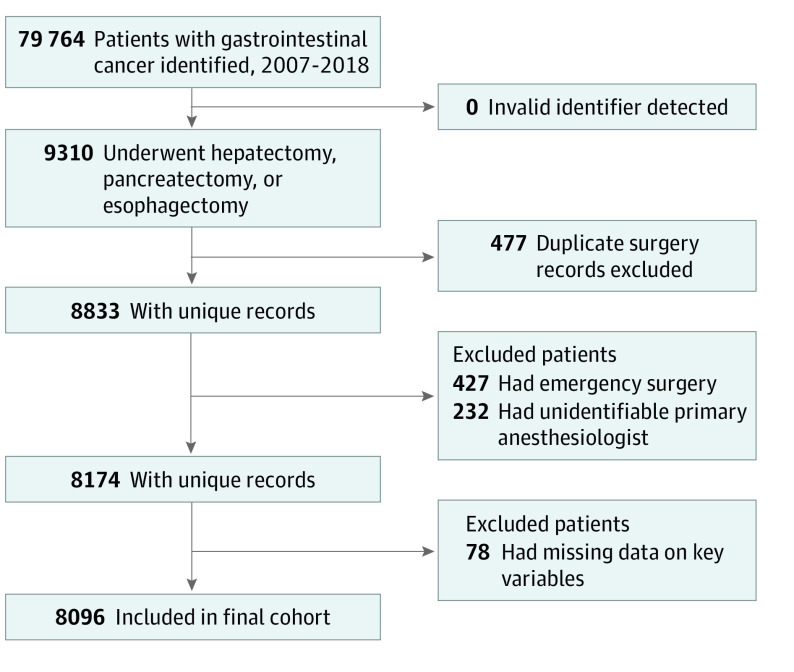
Design, setting, and participants: This population-based cohort study used administrative health care data sets from various data sources in Ontario, Canada. Adult patients who underwent esophagectomy, pancreatectomy, or hepatectomy for GI cancer from January 1, 2007, to December 31, 2018, were eligible. Patients with an invalid identification number, a duplicate surgery record, and missing primary anesthesiologist information were excluded.
Exposures: Primary anesthesiologist volume was defined as the annual number of procedures of interest (esophagectomy, pancreatectomy, and hepatectomy) supported by that anesthesiologist in the 2 years before the index surgery. Volume was dichotomized into low-volume and high-volume categories, with 75th percentile or 6 or more procedures per year selected as the cutoff point.
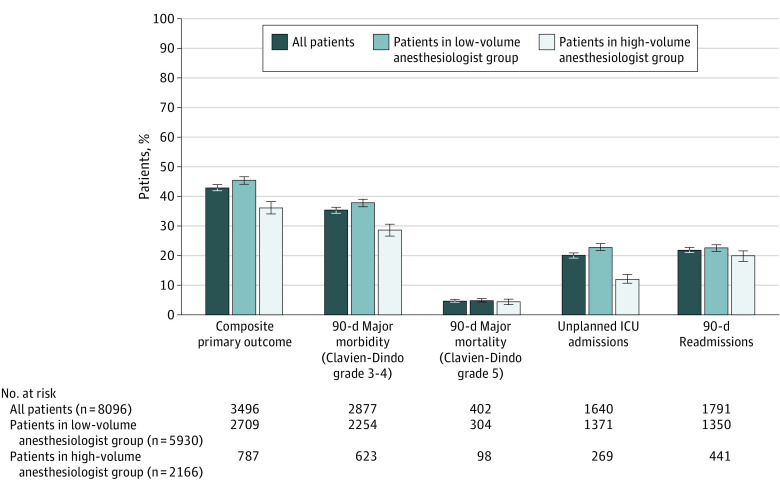
Main outcome and measures: The primary outcome was a composite of 90-day major morbidity (with a Clavien-Dindo classification grade 3-5) and readmission. Secondary outcomes were individual components of the primary outcome. The association between exposure and outcomes was examined using multivariable logistic regression models, accounting for potential confounders.
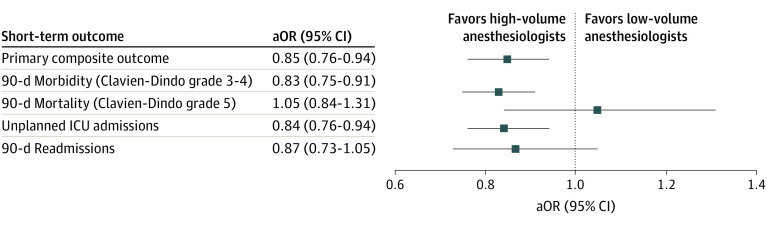
Results: Of the 8096 patients included, 5369 were men (66.3%) and the median (interquartile range [IQR]) age was 65 (57-72) years. Operations were supported by 842 anesthesiologists and performed by 186 surgeons, and the median (IQR) anesthesiologist volume was 3 (1.5-6) procedures per year. A total of 2166 patients (26.7%) received care from high-volume anesthesiologists. Primary outcome occurred in 36.3% of patients in the high-volume group and 45.7% of patients in the low-volume group. After adjustment, care by high-volume anesthesiologists was independently associated with lower odds of the primary outcome (adjusted odds ratio [aOR], 0.85; 95% CI, 0.76-0.94), major morbidity (aOR, 0.83; 95% CI, 0.75-0.91), unplanned intensive care unit admission (aOR, 0.84; 95% CI, 0.76-0.94), but not readmission (aOR, 0.87; 95% CI, 0.73-1.05) or mortality (aOR, 1.05; 95% CI, 0.84-1.31). E-values analysis indicated that an unmeasured variable would unlikely substantively change the observed risk estimates.
Conclusions and relevance: This study found that, among adults who underwent complex gastrointestinal cancer surgery, those who received care from high-volume anesthesiologists had a lower risk of adverse postoperative outcomes compared with those who received care from low-volume anesthesiologists. These findings support organizing perioperative care to increase anesthesiologist volume to optimize patient outcomes.
Conflict of interest statement
Figures

Comment in
-
Behind the Curtain-Implications of Anesthesia Volume on Outcomes.JAMA Surg. 2021 May 1;156(5):488. doi: 10.1001/jamasurg.2021.0136. JAMA Surg. 2021. PMID: 33729453 Free PMC article. No abstract available.
-
Socioeconomic Factors, Urological Epidemiology and Practice Patterns.J Urol. 2021 Dec;206(6):1507-1508. doi: 10.1097/JU.0000000000002221. Epub 2021 Sep 9. J Urol. 2021. PMID: 34496609 No abstract available.
-
Looking Over the Drape-Anesthesiologists' Volume and Surgical Outcomes.JAMA Surg. 2022 Jan 1;157(1):78-79. doi: 10.1001/jamasurg.2021.3755. JAMA Surg. 2022. PMID: 34586342 No abstract available.
-
Looking Over the Drape-Anesthesiologists' Volume and Surgical Outcomes-Reply.JAMA Surg. 2022 Jan 1;157(1):79. doi: 10.1001/jamasurg.2021.3756. JAMA Surg. 2022. PMID: 34586359 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
