

Learning from safety incidents in high-reliability organizations: a systematic review of learning tools that could be adapted and used in healthcare
- PMID: 33729493
- PMCID: PMC8271183
- DOI: 10.1093/intqhc/mzab046
Learning from safety incidents in high-reliability organizations: a systematic review of learning tools that could be adapted and used in healthcare
Abstract
Objective: A high-reliability organization (HRO) is an organization that has sustained almost error-free performance, despite operating in hazardous conditions where the consequences of errors could be catastrophic. A number of tools and initiatives have been used within HROs to learn from safety incidents, some of which have the potential to be adapted and used in healthcare. We conducted a systematic review to identify any learning tools deemed to be effective that could be adapted and used by multidisciplinary teams in healthcare following a patient safety incident.
Methods: This review followed the Preferred Reporting Items for Systematic Reviews and MetaAnalyses for Protocols reporting guidelines and was registered with the PROSPERO (CRD42017071528). A search of databases was carried out in January 2021, from the date of their commencement. We conducted a search on electronic databases such as Web of Science, Science Direct, MEDLINE in Process Jan 1950-present, EMBASE Jan 1974-present, CINAHL 1982-present, PsycINFO 1967-present, Scopus and Google Scholar. We also searched the grey literature including reports from government agencies, relevant doctoral dissertations and conference proceedings. A customized data extraction form was used to capture pertinent information from included studies and Critical Appraisal Skills Programme tool to appraise on their quality.
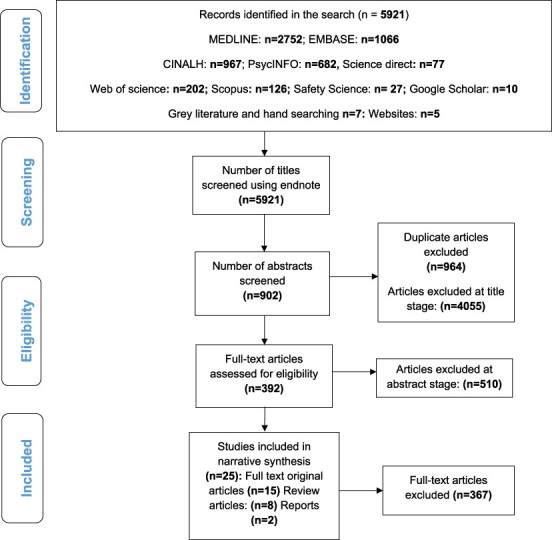
Results: A total of 5921 articles were identified, with 964 duplicate articles removed and 4932 excluded at the title (4055), abstract (510) and full-text (367) stages. Twenty-five articles were included in the review. Learning tools identified included debriefing, simulation, crew resource management and reporting systems to disseminate safety messages. Debriefing involved deconstructing incidents using reflective questions, whilst simulation training involved asking staff to relive the event again by performing the task(s) in a role-play scenario. Crew resource management is a set of training procedures that focus on communication, leadership and decision-making. Sophisticated incident-reporting systems provide valuable information on hazards and were widely recommended as a way of disseminating key safety messages following safety incidents. These learning tools were found to have a positive impact on learning if conducted soon after the incident with efficient facilitation.
Conclusion: Healthcare organizations should find ways to adapt to the learning tools or initiatives used in HROs following safety incidents. It is challenging to recommend any specific one as all learning tools have shown considerable promise. However, the way these tools or initiatives are implemented is critical, and so further work is needed to explore how to successfully embed them into healthcare organizations so that everyone at every level of the organization embraces them.
Keywords: after action review; crew resource management; debriefing; high-reliability organizations; safety incidents; simulation.
© The Author(s) 2021. Published by Oxford University Press on behalf of International Society for Quality in Health Care. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Beyond the black stump: rapid reviews of health research issues affecting regional, rural and remote Australia.Med J Aust. 2020 Dec;213 Suppl 11:S3-S32.e1. doi: 10.5694/mja2.50881. Med J Aust. 2020. PMID: 33314144
-
Factors influencing patient safety incident reporting in African healthcare organisations: a systematic integrative review.BMC Health Serv Res. 2025 Apr 30;25(1):619. doi: 10.1186/s12913-025-12762-1. BMC Health Serv Res. 2025. PMID: 40307741 Free PMC article.
-
Improving Incident Reporting in a Hospital-Based Radiation Oncology Department: The Impact of a Customized Crew Resource Training and Event Reporting Intervention.Cureus. 2021 Apr 5;13(4):e14298. doi: 10.7759/cureus.14298. Cureus. 2021. PMID: 33842178 Free PMC article.
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Systematic review of psychological, emotional and behavioural impacts of surgical incidents on operating theatre staff.BJS Open. 2017 Oct 26;1(4):106-113. doi: 10.1002/bjs5.21. eCollection 2017 Aug. BJS Open. 2017. PMID: 29951612 Free PMC article. Review.
Cited by
-
The analysis of collective orientation and process feedback in relation to coordination and performance in interdependently working teams.PLoS One. 2024 Mar 21;19(3):e0297565. doi: 10.1371/journal.pone.0297565. eCollection 2024. PLoS One. 2024. PMID: 38512956 Free PMC article.
-
Unsafe care in residential settings for older adults: a content analysis of accreditation reports.Int J Qual Health Care. 2023 Oct 26;35(4):mzad085. doi: 10.1093/intqhc/mzad085. Int J Qual Health Care. 2023. PMID: 37795694 Free PMC article.
-
The role of teamwork and non-technical skills for improving emergency surgical outcomes: an international perspective.Patient Saf Surg. 2022 Feb 8;16(1):8. doi: 10.1186/s13037-022-00317-w. Patient Saf Surg. 2022. PMID: 35135584 Free PMC article. Review.
-
Systematic review of types of safety incidents and the processes and systems used for safety incident reporting in care homes.J Adv Nurs. 2025 Jan;81(1):69-115. doi: 10.1111/jan.16264. Epub 2024 Jun 19. J Adv Nurs. 2025. PMID: 38895931 Free PMC article.
-
What digital health technology types are used in mental health prevention and intervention? Review of systematic reviews for systematization of technologies.J Occup Health. 2024 Jan 4;66(1):uiad003. doi: 10.1093/joccuh/uiad003. J Occup Health. 2024. PMID: 38258936 Free PMC article. Review.
References
-
- Bagnara S, Parlangeli O, Tartaglia R. Are hospitals becoming high reliability organizations? Appl Ergon 2010;41:713–8. - PubMed
-
- Cooke DL, Rohleder TR. Learning from incidents: from normal accidents to high reliability. Syst Dyn Rev 2006;22:213–39.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
