

Trends in Use of Low-Value Care in Traditional Fee-for-Service Medicare and Medicare Advantage
- PMID: 33729504
- PMCID: PMC7970337
- DOI: 10.1001/jamanetworkopen.2021.1762
Trends in Use of Low-Value Care in Traditional Fee-for-Service Medicare and Medicare Advantage
Abstract
Importance: Decreasing use of low-value care is a major goal for Medicare given the potential to decrease costs and harms. Compared with traditional fee-for-service Medicare (TM), Medicare Advantage (MA) is more strongly financially incentivized to decrease use of low-value care.
Objectives: To compare use of low-value care among individuals enrolled in TM and those enrolled in MA overall and to examine trends in use of low-value care in both programs from 2006 to 2015.
Design, setting, and participants: This cross-sectional study analyzed individuals enrolled in TM and MA using data from the 2006 to 2015 Medical Expenditure Panel Survey. To account for differences in characteristics between individuals enrolled in TM and those enrolled in MA, a propensity score-based approach was used. Data were analyzed from August 2020 through January 2021.
Exposures: Being enrolled in MA or TM.
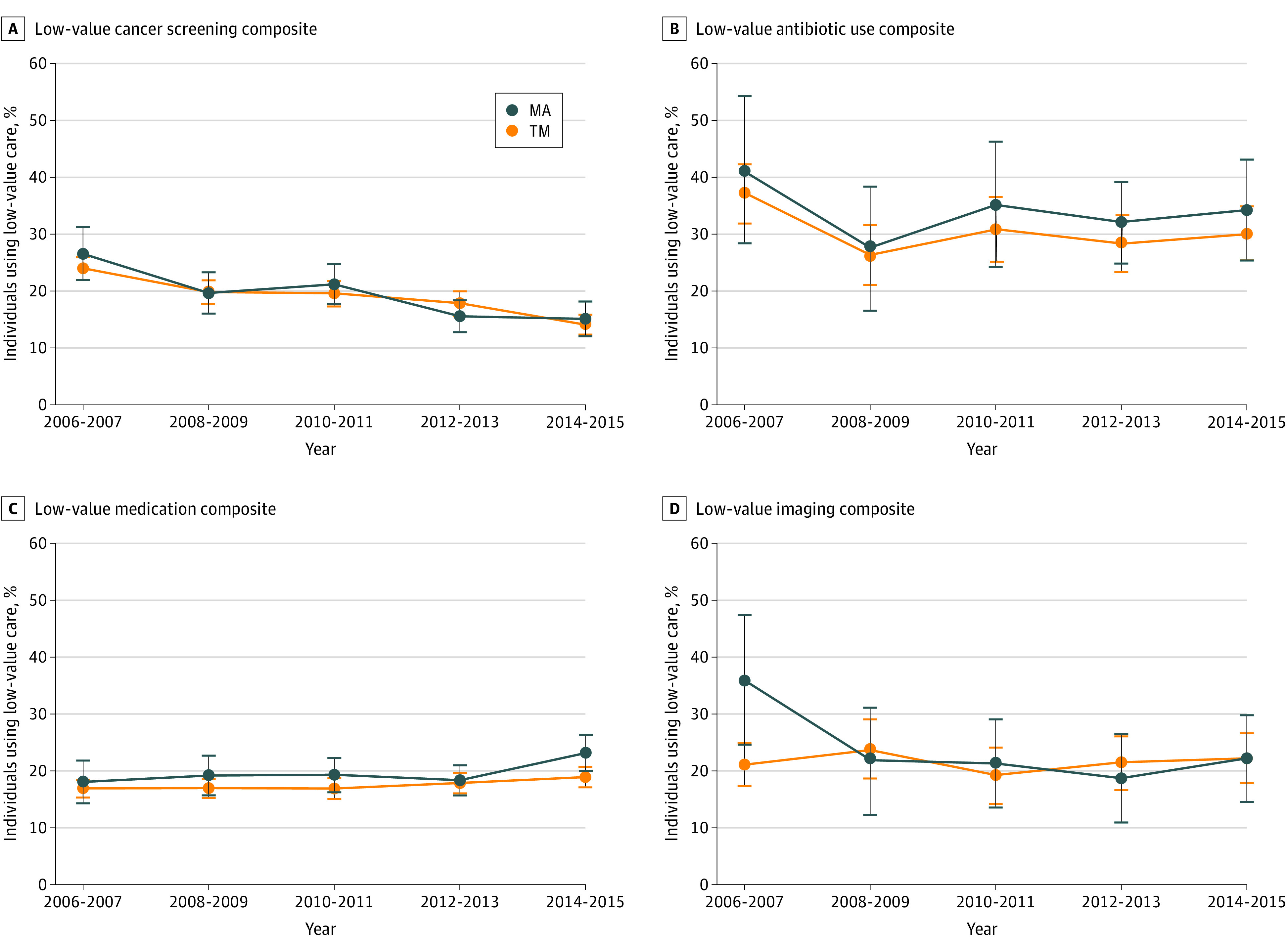
Main outcomes and measures: Binary measures of use were collected for 13 low-value services in 4 categories (ie, [1] cancer screening: cervical, colorectal, and prostate cancer screening in older adults; [2] antibiotic use: antibiotic for acute upper respiratory infection and antibiotic for influenza; [3] medication: anxiolytic, sedative, or hypnotic in an adult older than 65 years; benzodiazepine for depression; opioid for headache; opioid for back pain; and nonsteroidal anti-inflammatory drug [NSAID] for hypertension, heart failure, or chronic kidney disease; and [4] imaging: magnetic resonance imaging [MRI] or computed tomography [CT] for back pain, radiograph for back pain, and MRI or CT for headache) and 4 low-value composites corresponding to the categories (ie, cancer screening composite, antibiotic use composite, medication composite, and imaging composite).
Results: Among 11 677 individuals enrolled in TM and 5164 individuals enrolled in MA, 9429 (56.0%) were women and the mean (SD) age was 74.5 (6.3) years. Of 13 low-value services and 4 low-value composites, statistically significant differences were found in 2 measures. For the low-value medication composite, 2054 of 11 636 eligible individuals enrolled in TM (adjusted mean, 17.6%; 95% CI, 16.8%-18.3%) received the care, and 981 of 5141 eligible individuals enrolled in MA (adjusted mean, 19.7%; 95% CI, 18.3%-21.2%) received the care, for a rate of use that was significantly higher among individuals enrolled in MA, by 2.2 percentage points (95% CI, 0.5-3.8 percentage points; P = .02). For the NSAID use for hypertension, heart failure, or kidney disease metric, 807 of 7832 individuals enrolled in TM (adjusted mean, 10.0%; 95% CI, 9.2%-10.8%) received the care, and 447 of 3566 individuals enrolled in MA (adjusted mean, 12.9%; 95% CI, 19.7%-27.1%) received the care, for a rate of use that was significantly higher among individuals enrolled in MA, by 2.9 percentage points (95% CI, 1.3-4.6 percentage points; P = .001). Overall, there were no decreases in use of low-value care in TM or MA over time.
Conclusions and relevance: This cross-sectional study found that use of low-value care was similarly prevalent in MA and TM, suggesting that MA enrollment was not associated with decreased provision of low-value care compared with TM.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
