

Chicago classification version 4.0© technical review: Update on standard high-resolution manometry protocol for the assessment of esophageal motility
- PMID: 33729668
- PMCID: PMC8268048
- DOI: 10.1111/nmo.14120
Chicago classification version 4.0© technical review: Update on standard high-resolution manometry protocol for the assessment of esophageal motility
Abstract
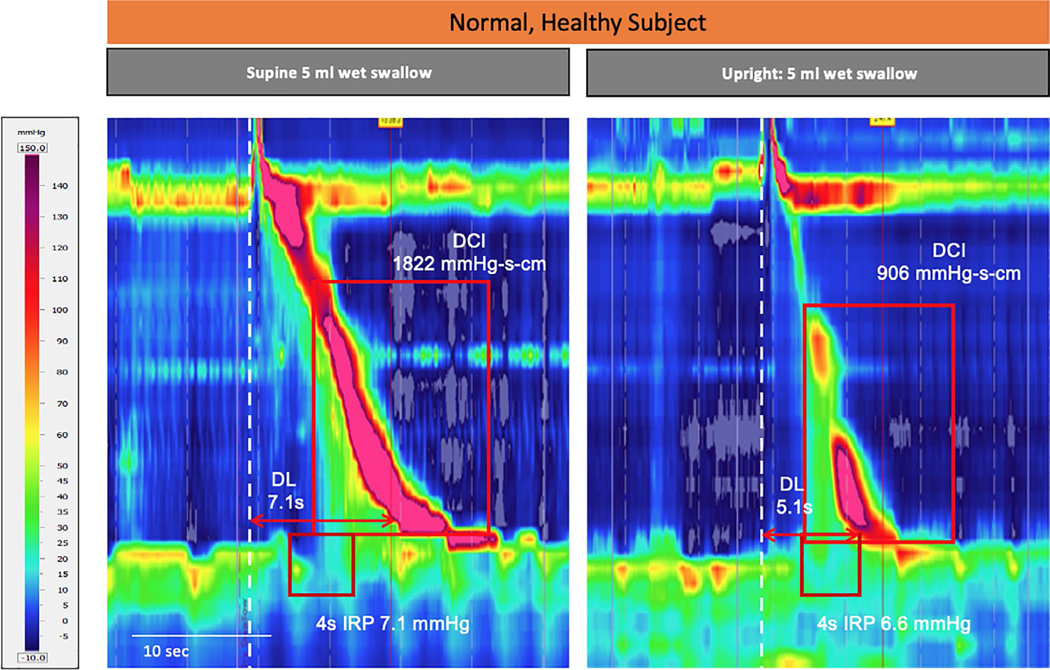
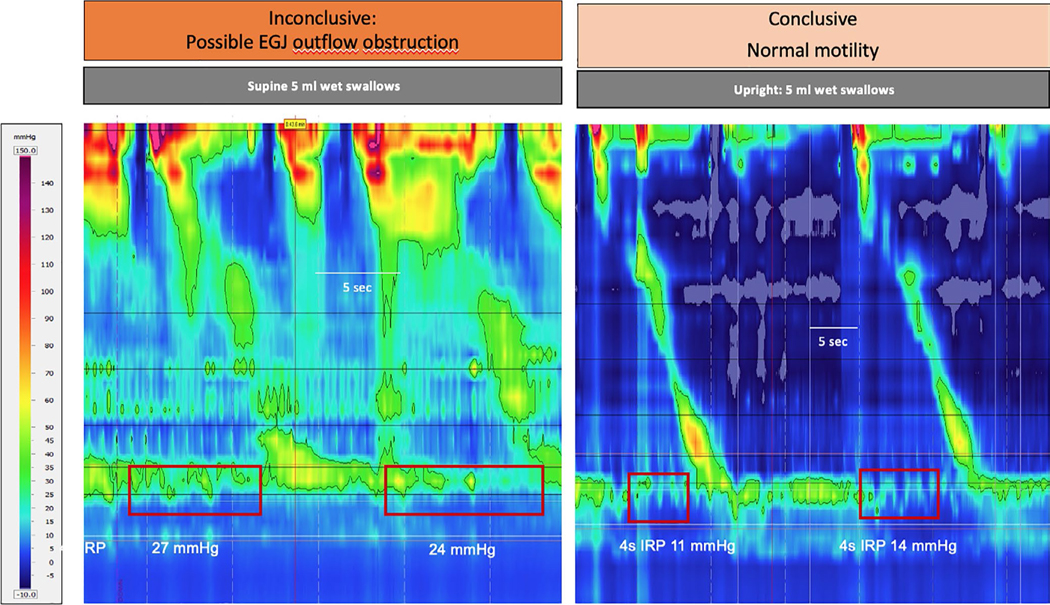
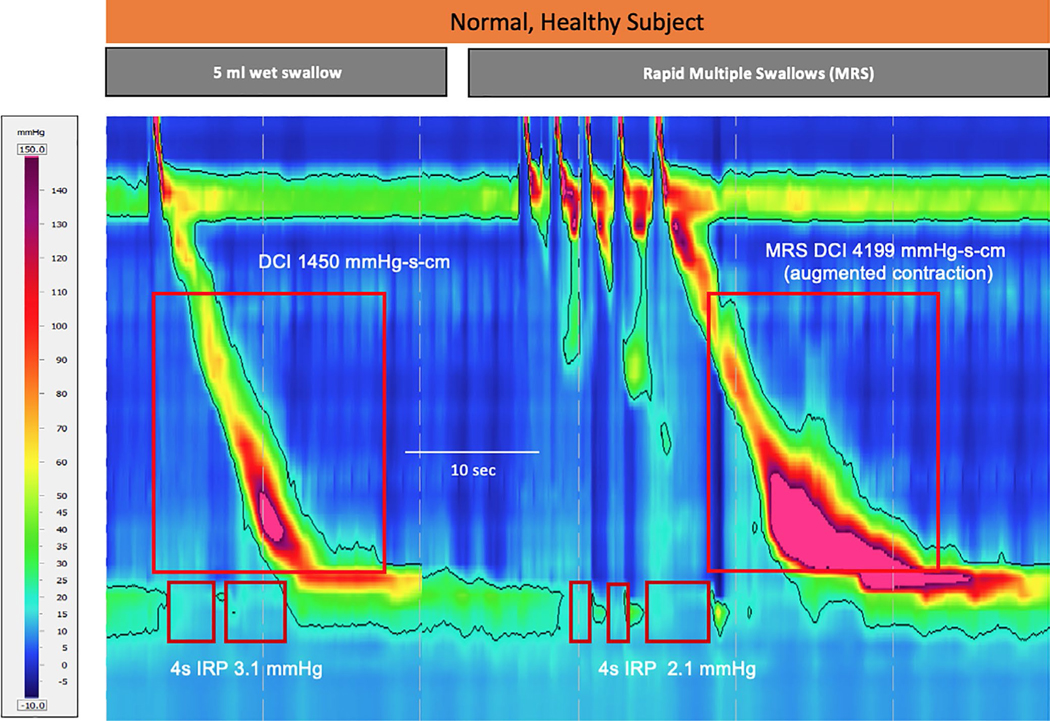
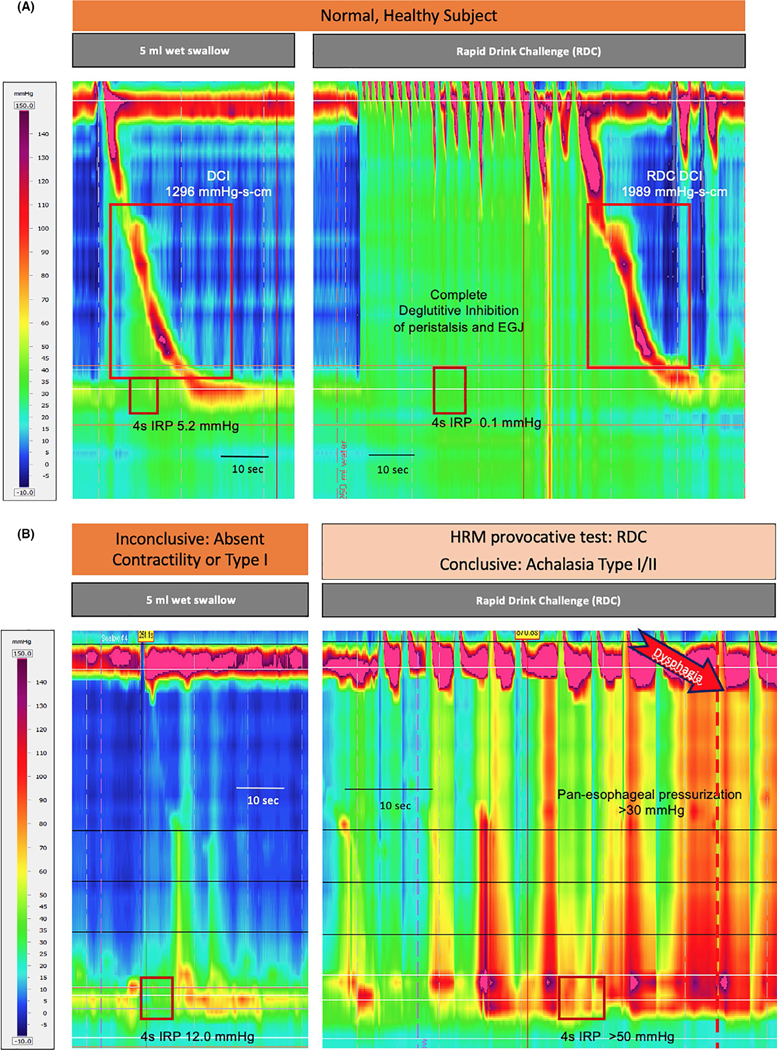
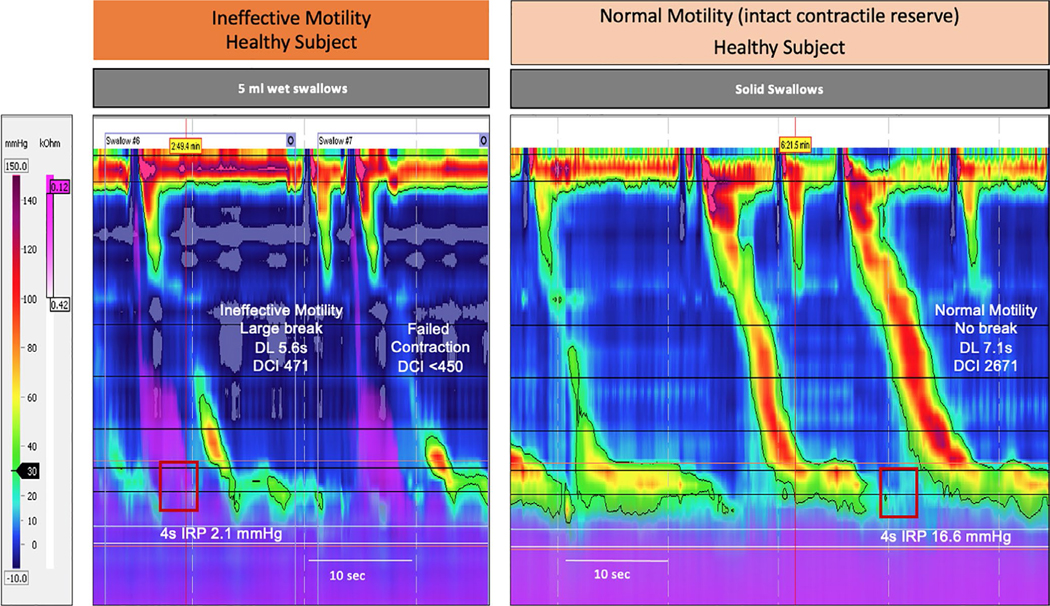
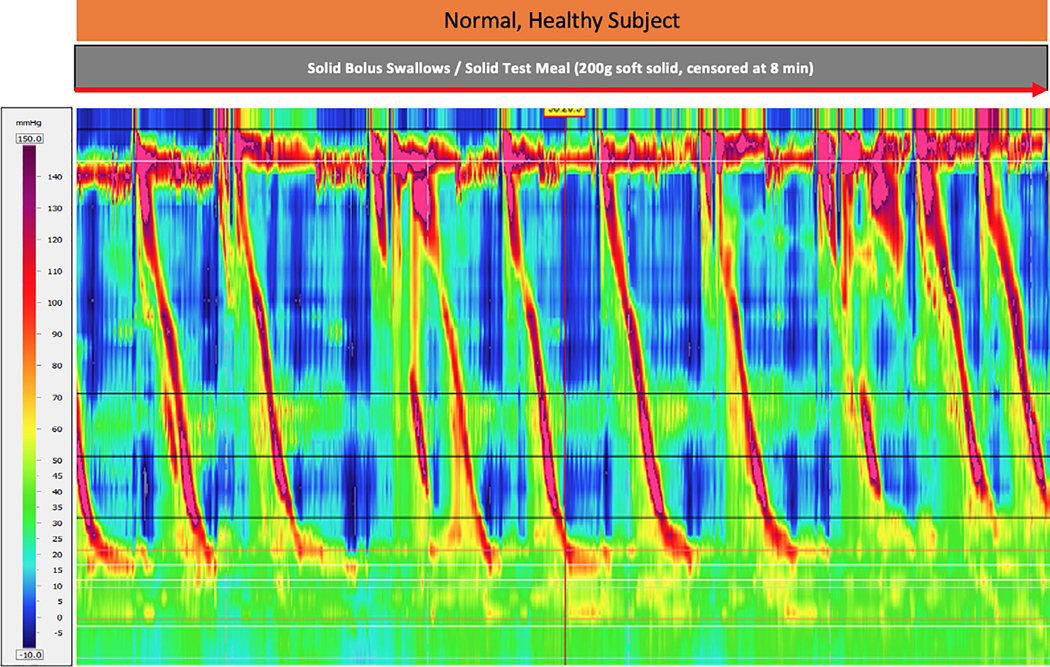
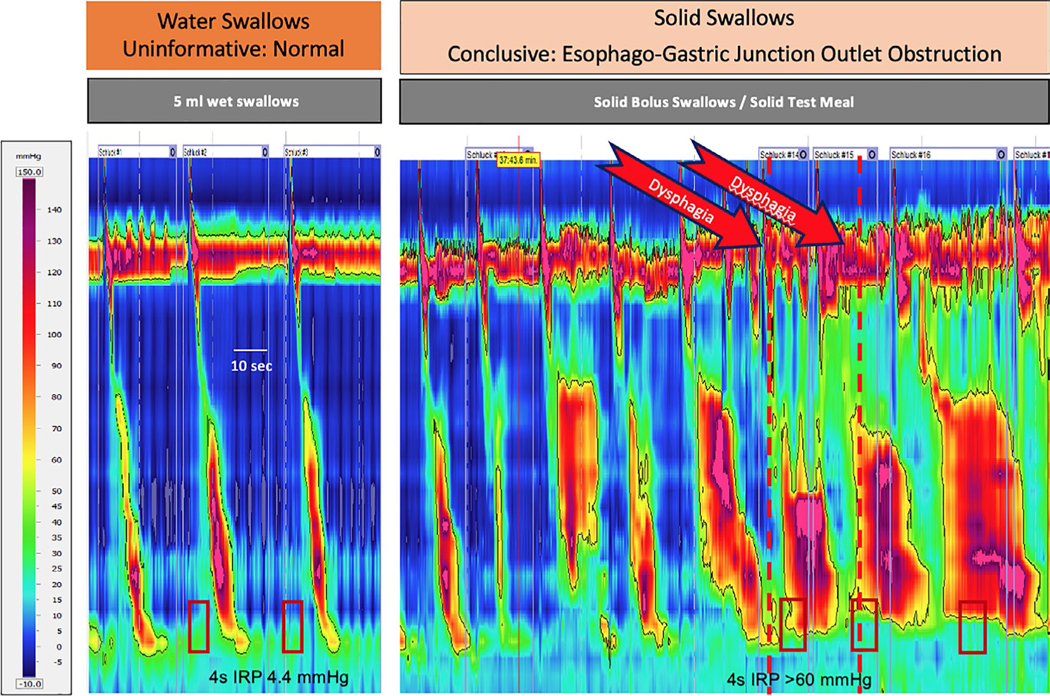
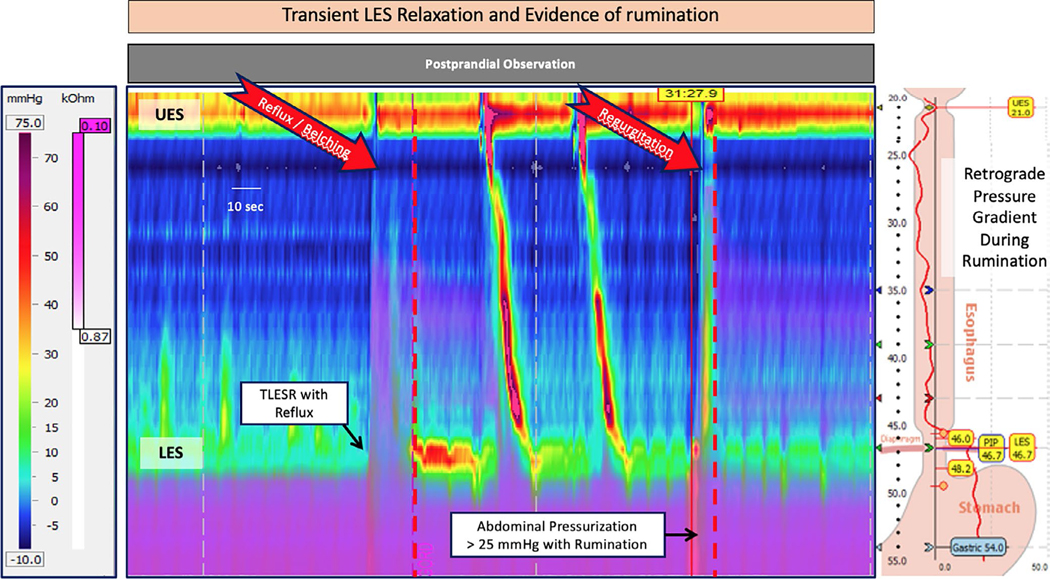
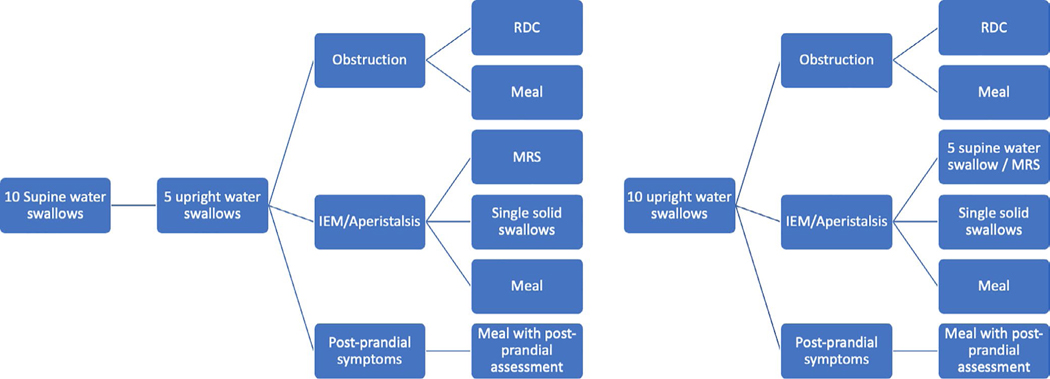
The Chicago Classification v4.0 (CCv4.0) is the updated classification scheme for esophageal motility disorders using metrics from high-resolution manometry (HRM). A key feature of CCv.4.0 is the more rigorous and expansive protocol that incorporates single wet swallows acquired in different positions (supine, upright) and provocative testing, including multiple rapid swallows and rapid drink challenge. Additionally, solid bolus swallows, solid test meal, and/or pharmacologic provocation can be used to identify clinically relevant motility disorders and other conditions (eg, rumination) that occur during and after meals. The acquisition and analysis for performing these tests and the evidence supporting their inclusion in the Chicago Classification protocol is detailed in this technical review. Provocative tests are designed to increase the diagnostic sensitivity and specificity of HRM studies for disorders of esophageal motility. These changes attempt to minimize ambiguity in prior iterations of Chicago Classification, decrease the proportion of HRM studies that deliver inconclusive diagnoses and increase the number of patients with a clinically relevant diagnosis that can direct effective therapy. Another aim in establishing a standard manometry protocol for motility laboratories around the world is to facilitate procedural consistency, improve diagnostic reliability, and promote collaborative research.
© 2021 John Wiley & Sons Ltd.
Conflict of interest statement
CONFLICT OF INTEREST
Other authors have none to report.
Figures
References
-
- Fox MR, Kahrilas PJ, Roman S, et al. Clinical measurement of gastrointestinal motility and function: who, when and which test? Nat Rev Gastroenterol Hepatol. 2018;15:568–579. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
