

Persistent Disparity: Socioeconomic Deprivation and Cancer Outcomes in Patients Treated in Clinical Trials
- PMID: 33729825
- PMCID: PMC8078474
- DOI: 10.1200/JCO.20.02602
Persistent Disparity: Socioeconomic Deprivation and Cancer Outcomes in Patients Treated in Clinical Trials
Abstract
Purpose: Patients with cancer living in socioeconomically disadvantaged areas have worse cancer outcomes. The association between socioeconomic deprivation and outcomes among patients with cancer participating in clinical trials has not been systematically examined.
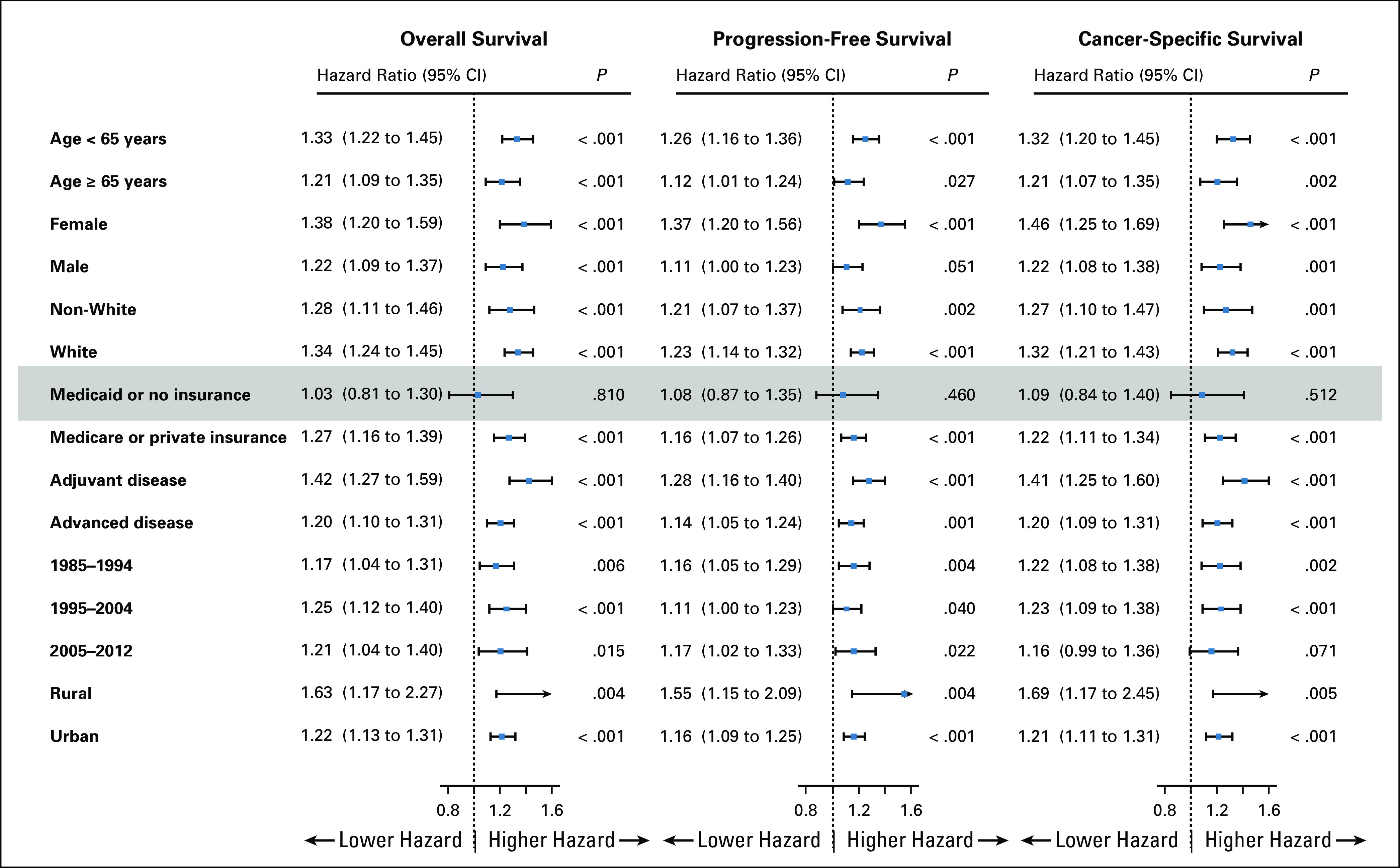
Methods: We examined survival outcomes for patients enrolled in phase III and large phase II clinical trials for major cancers conducted by the SWOG Cancer Research Network from 1985 to 2012. Socioeconomic deprivation was measured using trial participants' residential zip codes linked to the Area Deprivation Index (ADI). Five-year overall survival, progression-free survival, and cancer-specific survival were examined using Cox regression frailty models, adjusting for age, sex, and race, and separately for insurance status, prognostic risk, and rural or urban residency.
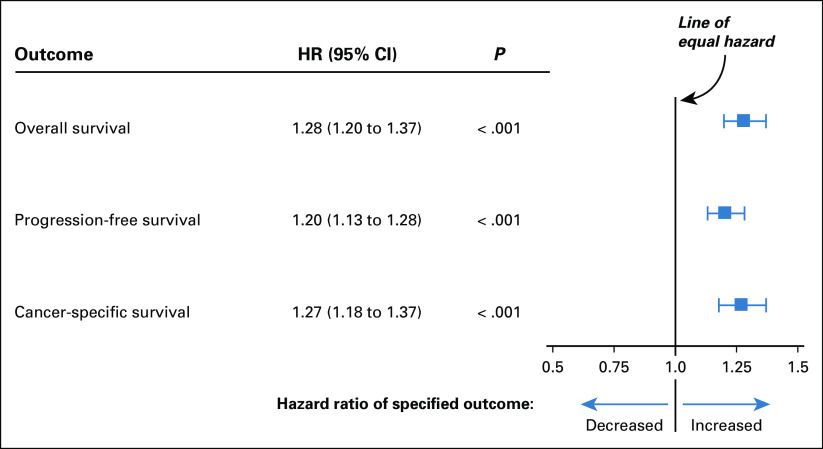
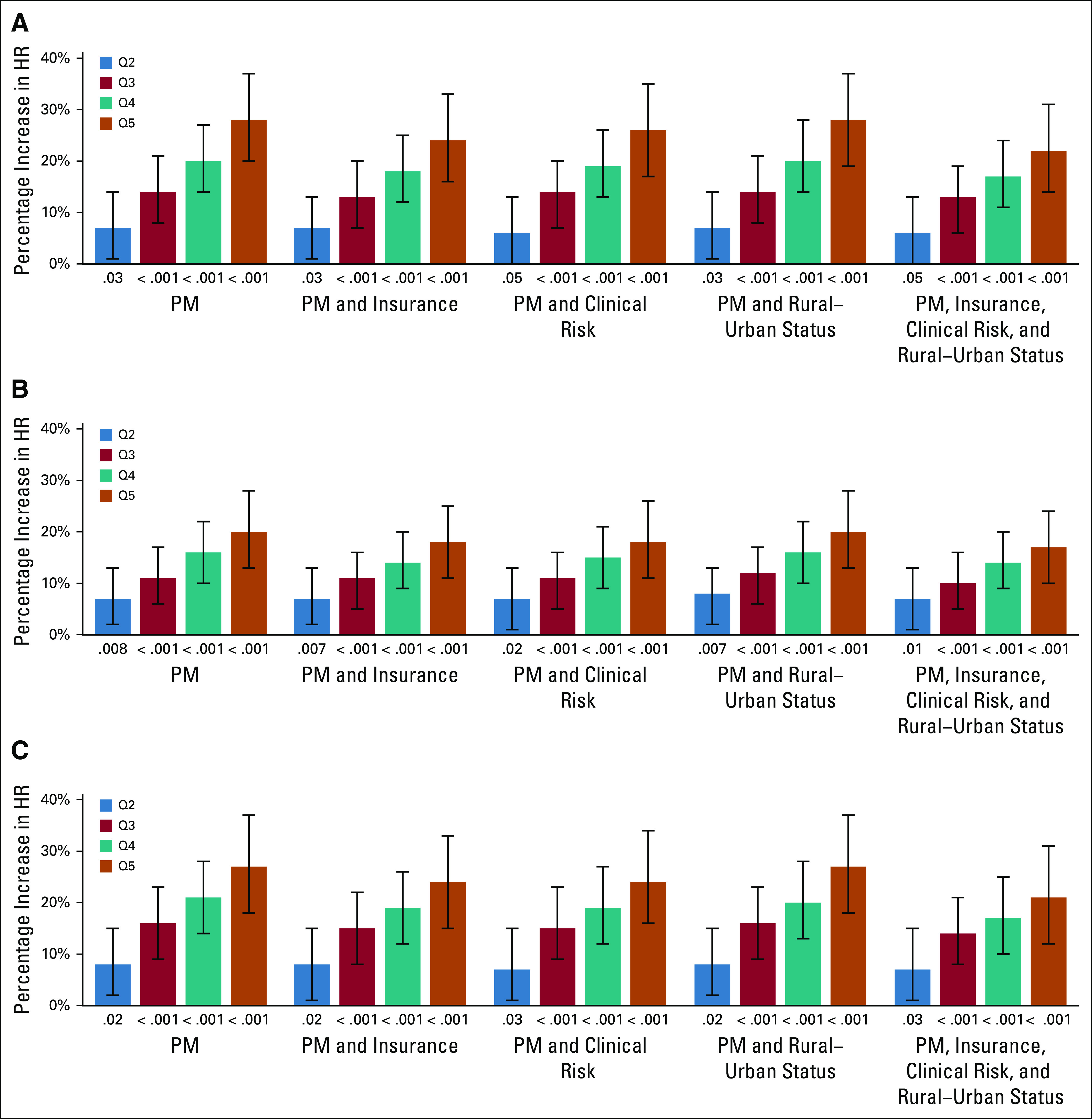
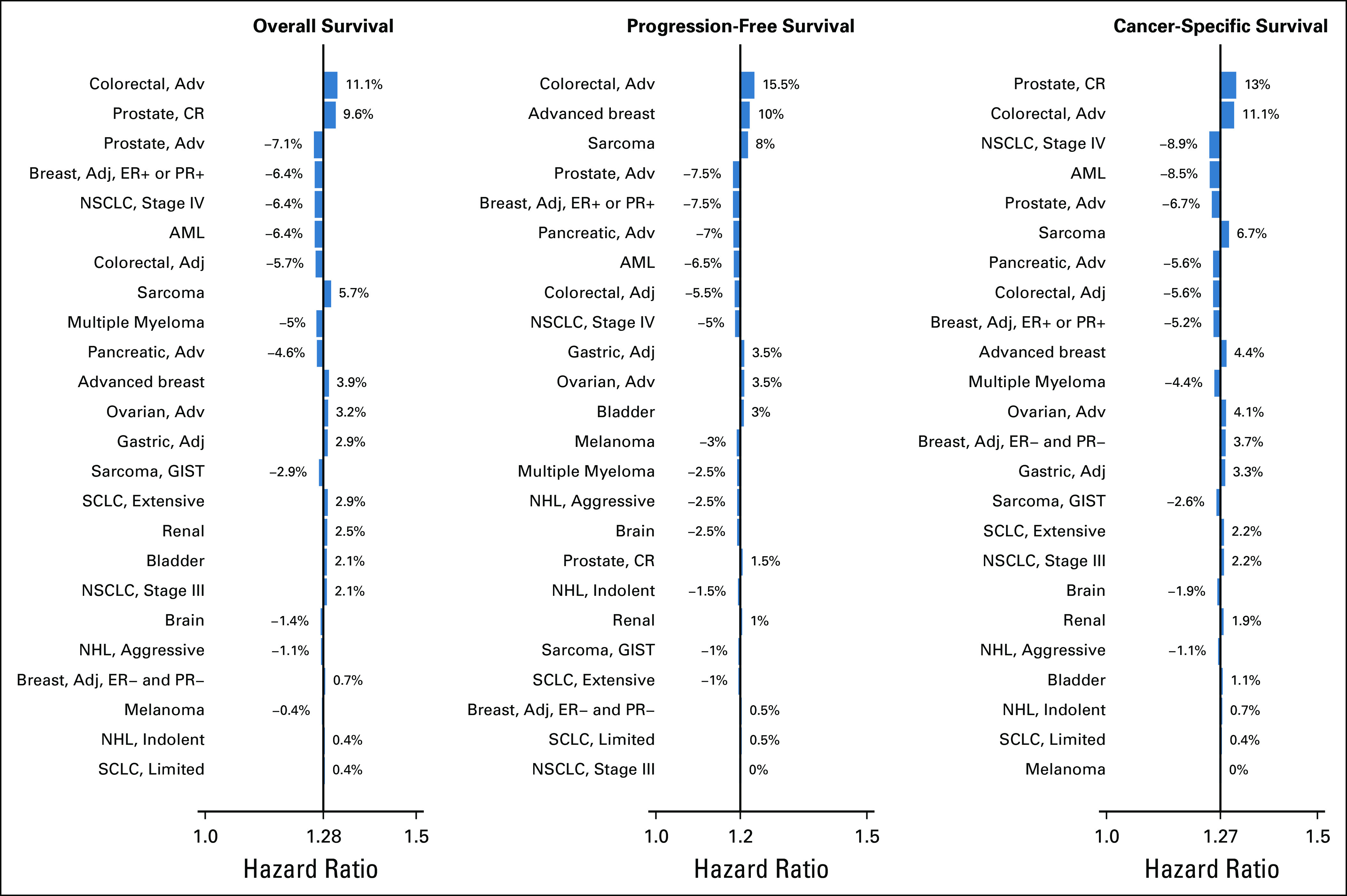
Results: We examined 41,109 patients from 55 trials comprising 24 cancer histology and stage-specific cohorts. Compared with trial participants in the most affluent areas (ADI, 0%-20%), trial participants from areas with the highest socioeconomic deprivation (ADI, 80%-100%) had worse overall (hazard ratio [HR] = 1.28, 95% CI, 1.20 to 1.37, P < .001), progression-free (HR = 1.20, 95% CI, 1.13 to 1.28, P < .001), and cancer-specific survival (HR = 1.27, 95% CI, 1.18 to 1.37, P < .001). The results were similar after adjusting for insurance status, prognostic risk, and rural or urban residency. There was a continuous increase in risk of all outcomes as the ADI quintile increased.
Conclusion: In patients with cancer with access to protocol-directed care in clinical trials, high area-level socioeconomic deprivation was associated with worse survival. Future research should examine whether the etiology of this residual disparity is related to reduced access to supportive care or postprotocol therapy and/or to differences in health status not reflected by protocol selection criteria.
Conflict of interest statement
Figures
References
-
- Link BG, Phelan J: Social conditions as fundamental causes of disease. J Health Soc Behav 80-94, 1995 - PubMed
-
- Chen E, Miller GE: Socioeconomic status and health: Mediating and moderating factors. Annu Rev Clin Psychol 9:723-749, 2013 - PubMed
-
- Cutler DM, Lleras-Muney A, Vogl T: Socioeconomic status and health: Dimensions and mechanisms. NBER Working Paper No. 14333. 2008.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
