

Needle in the heart: a rare case of cardiac tamponade caused by a migrated foreign body and mimicking ST segment elevation myocardial infarction
- PMID: 33730997
- PMCID: PMC7972190
- DOI: 10.1186/s12872-021-01950-6
Needle in the heart: a rare case of cardiac tamponade caused by a migrated foreign body and mimicking ST segment elevation myocardial infarction
Abstract
Background: Pericardial tamponade is a serious condition which may eventually lead to severe haemodynamic disturbances and cardiac arrest. It is most often caused by the accumulation of fluid inside the pericardium, as a result of different aetiological factors such as pericarditis, neoplastic diseases, lymphatic dysfunctions, or idiopathic pericardial disease. Pericardial tamponade can develop after cardiac surgical procedures or as a complication of myocardial infarction. Collection of blood inside the pericardial sack can be the result of pericardial or cardiac trauma. It is exceedingly rare for the injury to be caused by a migrating foreign body. Although a typical picture of pericardial tamponade has been previously described, the disorder may clinically resemble an acute myocardial infarction.
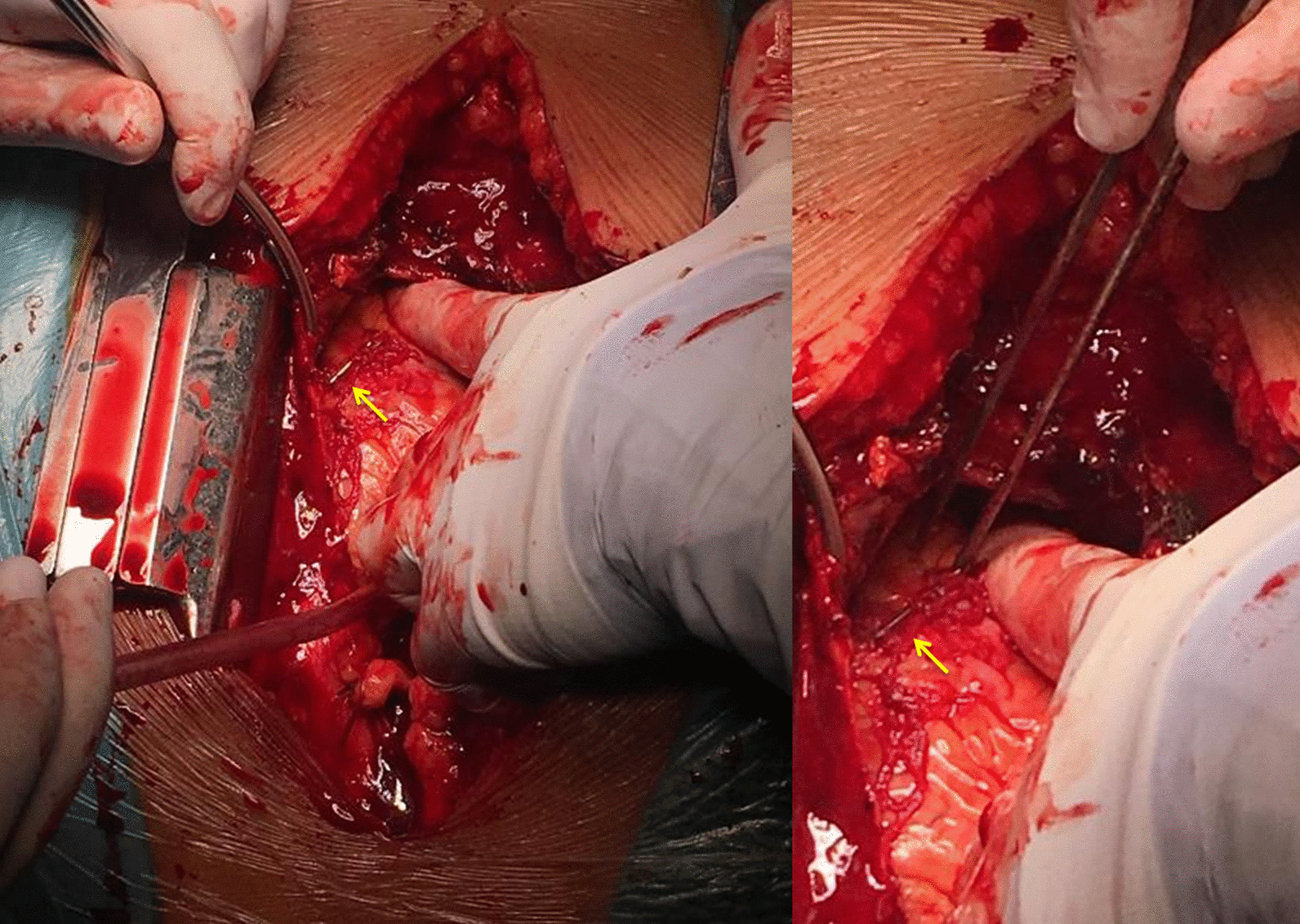
Case presentation: We report the case of a 58-year-old female patient complaining of new onset thoracic pain and shortness of breath. Electrocardiographic examination results were suggestive of an acute inferior myocardial infarction. However, echocardiography revealed significant pericardial tamponade. The cause was found to be a needle which remained inside the pelvis following a previous cesarean delivery, which the patient had undergone 18 years prior. In emergency setting, the needle was removed and the pericardial tamponade was resolved. Due to the prompt and efficient management, the patient had an uneventful postoperative recovery and presented no recurrence at the follow-up examinations.
Conclusions: The migration of foreign bodies through tissues is exceedingly rare. If present, it may cause life-threatening complications. Since the aetiology of pericardial tamponade is vast, a thorough assessment is highly important. Therefore, echocardiography is the imaging modality of choice. We wish to highlight the possibility of migrating foreign bodies as probable cause for pericardial tamponade, as well as the importance of echocardiographic methods in the fast-track evaluation of such critical conditions.
Keywords: Cardiac tamponade; Case report; Foreign body migration; STEMI.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
-
- Beck CS. Two cardiac compression triads. JAMA. 1935;104(9):714–716. doi: 10.1001/jama.1935.02760090018005. - DOI
-
- Arafat Amr A, Taha Abdel-Hady M, Elkhouly Ahmed G, Elgalad AA. Can a foreign body migrate against natural body barriers? Ann Pediatric Surg. 2017;13(3):157–159. doi: 10.1097/01.XPS.0000508438.29481.2e. - DOI
-
- Ibanez B, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC) Eur Heart J. 2018;39(2):119–177. doi: 10.1093/eurheartj/ehx393. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
