

Characteristics of patients with Coronavirus Disease 2019 (COVID-19) and seasonal influenza at time of hospital admission: a single center comparative study
- PMID: 33731019
- PMCID: PMC7968573
- DOI: 10.1186/s12879-021-05957-4
Characteristics of patients with Coronavirus Disease 2019 (COVID-19) and seasonal influenza at time of hospital admission: a single center comparative study
Abstract
Background: In the future, co-circulation of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and influenza viruses A/B is likely. From a clinical point of view, differentiation of the two disease entities is crucial for patient management. We therefore aim to detect clinical differences between Coronavirus Disease 2019 (COVID-19) and seasonal influenza patients at time of hospital admission.
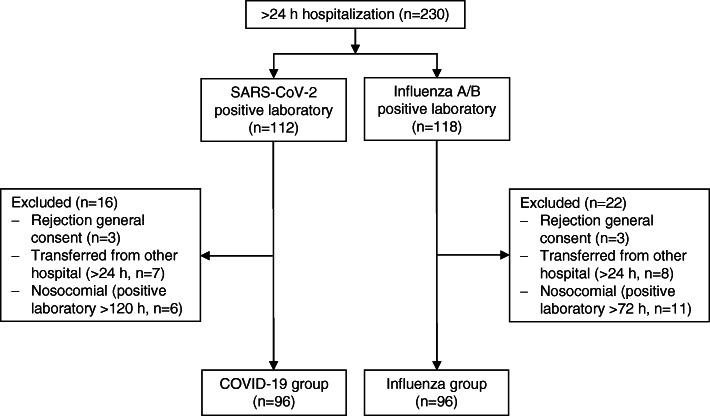
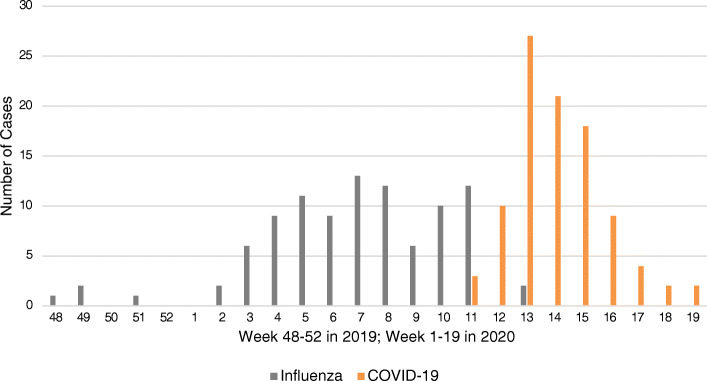
Methods: In this single-center observational study, we included all consecutive patients hospitalized for COVID-19 or influenza between November 2019 and May 2020. Data were extracted from a nationwide surveillance program and from electronic health records. COVID-19 and influenza patients were compared in terms of baseline characteristics, clinical presentation and outcome. We used recursive partitioning to generate a classification tree to discriminate COVID-19 from influenza patients.
Results: We included 96 COVID-19 and 96 influenza patients. Median age was 68 vs. 70 years (p = 0.90), 72% vs. 56% (p = 0.024) were males, and median Charlson Comorbidity Index (CCI) was 1 vs. 2 (p = 0.027) in COVID-19 and influenza patients, respectively. Time from symptom onset to hospital admission was longer for COVID-19 (median 7 days, IQR 3-10) than for influenza patients (median 3 days, IQR 2-5, p < 0.001). Other variables favoring a diagnosis of COVID-19 in the classification tree were higher systolic blood pressure, lack of productive sputum, and lack of headache. The tree classified 86/192 patients (45%) into two subsets with ≥80% of patients having influenza or COVID-19, respectively. In-hospital mortality was higher for COVID-19 patients (16% vs. 5%, p = 0.018).
Conclusion: Discriminating COVID-19 from influenza patients based on clinical presentation is challenging. Time from symptom onset to hospital admission is considerably longer in COVID-19 than in influenza patients and showed the strongest discriminatory power in our classification tree. Although they had fewer comorbidities, in-hospital mortality was higher for COVID-19 patients.
Keywords: COVID-19; Classification tree; Comparative; Differences; Influenza; SARS-CoV-2.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Li Y, Reeves RM, Wang X, Bassat Q, Brooks WA, Cohen C, et al. Global patterns in monthly activity of influenza virus, respiratory syncytial virus, parainfluenza virus, and metapneumovirus: a systematic analysis. Lancet Glob Health. 2019;7(8):e1031–e1045. doi: 10.1016/S2214-109X(19)30264-5. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
