

Weight gain after diagnosis of gestational diabetes mellitus and its association with adverse pregnancy outcomes: a cohort study
- PMID: 33731035
- PMCID: PMC7971950
- DOI: 10.1186/s12884-021-03690-z
Weight gain after diagnosis of gestational diabetes mellitus and its association with adverse pregnancy outcomes: a cohort study
Abstract
Background: Gestational diabetes mellitus (GDM) and excessive body weight are two key risk factors for adverse perinatal outcomes. However, it is not clear whether restricted gestational weight gain (GWG) is favorable to reduce the risk for adverse pregnancy and neonatal outcomes in women with GDM. Therefore, this study aimed to assess the association of GWG after an oral glucose tolerance test with maternal and neonatal outcomes.
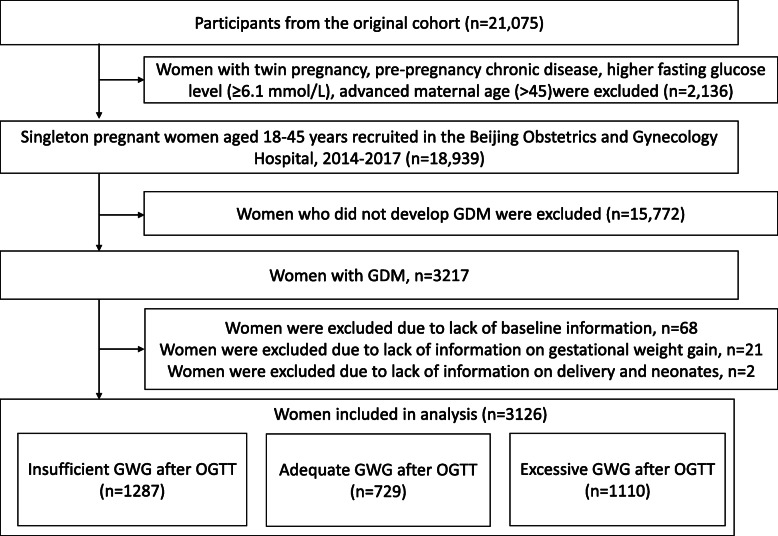
Methods: This prospective cohort study assessed the association of GWG after an oral glucose tolerance test (OGTT) with pregnancy and neonatal outcomes in 3126 women with GDM, adjusted for age, pre-pregnancy body mass index, height, gravidity, parity, adverse history of pregnancy, GWG before OGTT, blood glucose level at OGTT and late pregnancy. The outcomes included the prevalence of pregnancy-induced hypertension (PIH) and preeclampsia, large for gestational age (LGA), small for gestational age, macrosomia, low birth weight, preterm birth, and birth by cesarean section. GDM was diagnosed according to the criteria established by the International Association of Diabetes and Pregnancy Study Groups.
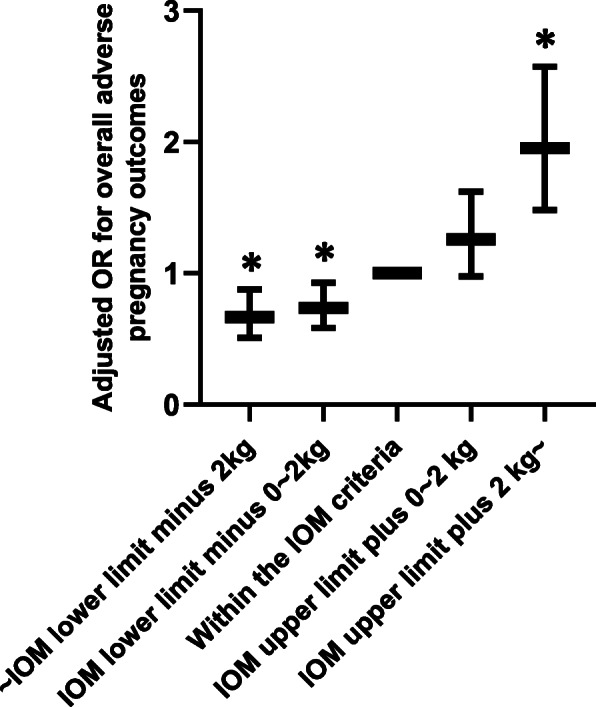
Results: GWG after OGTT was positively associated with risk for overall adverse pregnancy outcomes (adjusted odds ratio [aOR] = 1.72, 95% confidence interval [CI] = 1.50-1.97), LGA (aOR = 1.29, 95%CI = 1.13-1.47), macrosomia (aOR = 1.24, 95%CI = 1.06-1.46) and birth by cesarean section (aOR = 1.91, 95%CI = 1.67-2.19) in women with GDM. Further analyses revealed that a combination of excessive GWG before OGTT and after OGTT increased the risk of PIH and preeclampsia, LGA, macrosomia, and birth by cesarean section compared with adequate GWG throughout pregnancy. In contrast, GWG below the Institute of Medicine guideline after OGTT did not increase the risk of adverse perinatal outcomes despite GWG before OGTT.
Conclusion: Excessive GWG after OGTT was associated with an elevated risk of adverse pregnancy outcomes, while insufficient GWG after OGTT did not increase the risk of LBW. Restricting GWG after diagnosis of GDM in women with excessive GWG in the first half of pregnancy may be beneficial to prevent PIH and preeclampsia, LGA, macrosomia, and birth by cesarean section.
Keywords: Gestational diabetes mellitus; Gestational weight gain; Neonatal outcomes; Oral glucose tolerance test; Pregnancy outcome.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- International Association of Diabetes Pregnancy Study Groups Consensus Panel. Metzger BE, Gabbe SG, Persson B, Buchanan TA, Catalano PA, Damm P, Dyer AR, Leiva A, Hod M, et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care. 2010;33(3):676–682. doi: 10.2337/dc09-1848. - DOI - PMC - PubMed
-
- Wendland EM, Torloni MR, Falavigna M, Trujillo J, Dode MA, Campos MA, Duncan BB, Schmidt MI. Gestational diabetes and pregnancy outcomes--a systematic review of the World Health Organization (WHO) and the International Association of Diabetes in Pregnancy Study Groups (IADPSG) diagnostic criteria. BMC Pregnancy Childbirth. 2012;12:23. doi: 10.1186/1471-2393-12-23. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
