

Usefulness of monitoring circulating tumor cells as a therapeutic biomarker in melanoma with BRAF mutation
- PMID: 33731038
- PMCID: PMC7968258
- DOI: 10.1186/s12885-021-08016-y
Usefulness of monitoring circulating tumor cells as a therapeutic biomarker in melanoma with BRAF mutation
Abstract
Background: While molecularly targeted therapies and immune checkpoint inhibitors have improved the prognosis of advanced melanoma, biomarkers are required to monitor drug responses. Circulating tumor cells (CTCs) are released from primary and/or metastatic tumors into the peripheral blood. We examined whether CTCs have potential as biomarkers by checking the number of CTCs, as well as the BRAF genotype of individual CTCs, in melanoma patients undergoing BRAF/MEK inhibitor treatment.
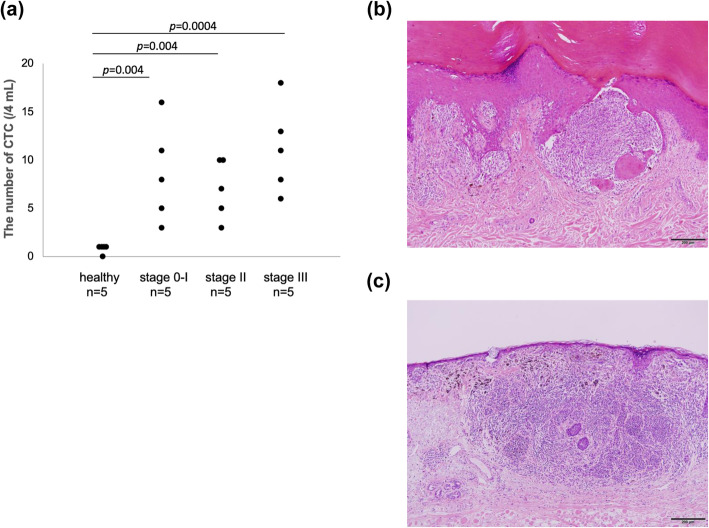
Methods: CTCs were isolated from peripheral blood using a high-density dielectrophoretic microwell array, followed by labeling with melanoma-specific markers (MART-1 and/or gp100) and a leukocyte marker (CD45). The numbers of CTCs were analyzed in fifteen patients with stage 0-III melanoma. Furthermore, changes in CTC numbers were assessed in five patients with stage IV melanoma at four time points during BRAF/MEK inhibitor treatment, and the BRAF genotype was analyzed in CTCs isolated from one patient.
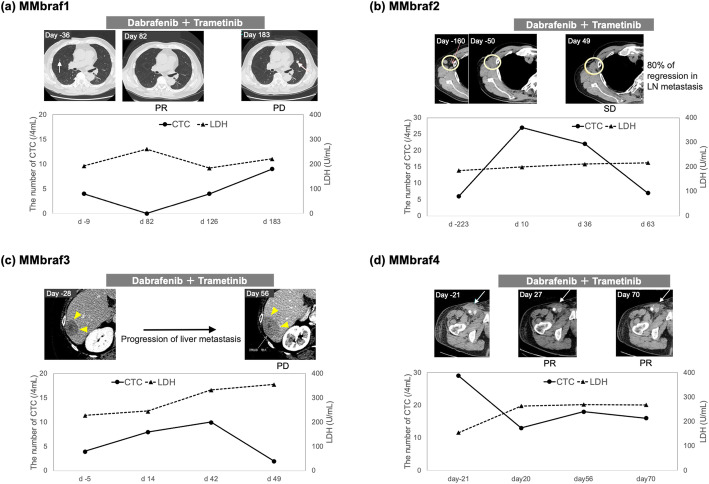
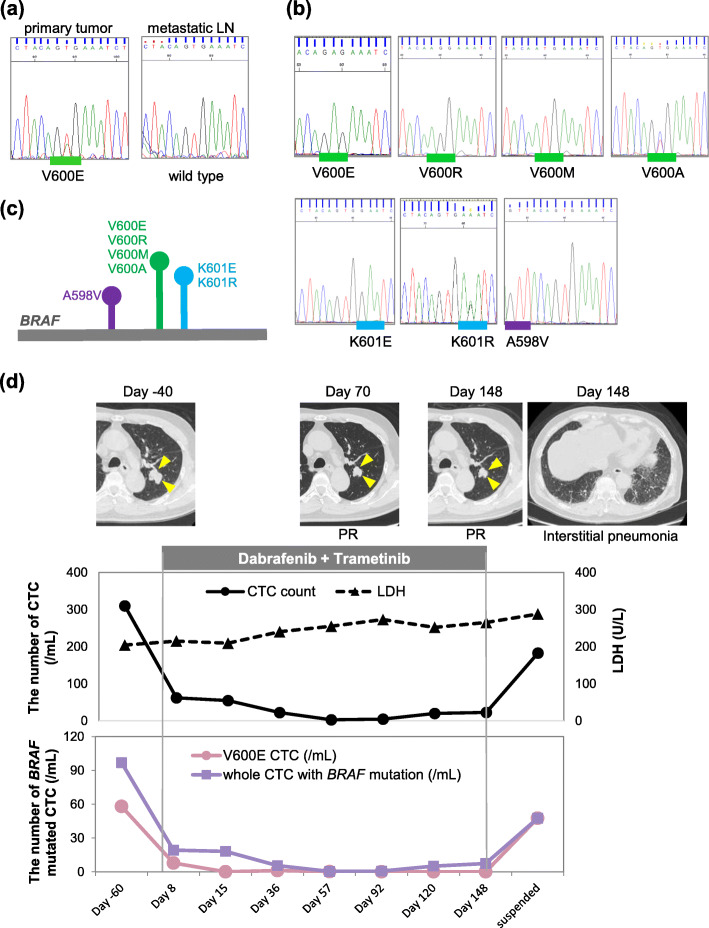
Results: We examined CTCs in patients with stage 0-III (five samples per stage: stage 0-I, stage II, and stage III), and detected CTCs even in patients with early disease (stage 0 and I). Interestingly, recurrence occurred in the lymph nodes of one stage I patient 2 years after the detection of a high number of CTCs in the patient's blood. The total number of CTCs in four of five patients with stage IV melanoma fluctuated in response to BRAF/MEK inhibitor treatment, suggesting that CTC number has potential for use as a drug response marker in advanced disease patients. Interestingly, one of those patients had CTCs harboring seven different BRAF genotypes, and the mutated CTCs disappeared upon BRAF/MEK inhibitor treatment, except for those harboring BRAFA598V.
Conclusions: CTCs are present even in the early stage of melanoma, and the number of CTCs seems to reflect patients' responses to BRAF/MEK inhibitor treatment. Furthermore, genetic heterogeneity of BRAF may contribute to resistance to BRAF/MEK inhibitors. Our findings demonstrate the usefulness of CTC analysis for monitoring responses to targeted therapies in melanoma patients, and for understanding the mechanism of drug resistance.
Keywords: BRAF; BRAF/MEK inhibitor; Circulating tumor cell; Heterogenous mutation; Melanoma.
Conflict of interest statement
Y.A. and A.M. are employees of Tosoh. Tosoh has applied for patents related to the dielectrophoretic microwell array system. This does not alter the authors’ adherence to all the policies of
Figures
References
-
- Robert C, Grob JJ, Stroyakovskiy D, Karaszewska B, Hauschild A, Levchenko E, Chiarion Sileni V, Schachter J, Garbe C, Bondarenko I, Gogas H, Mandalá M, Haanen JBAG, Lebbé C, Mackiewicz A, Rutkowski P, Nathan PD, Ribas A, Davies MA, Flaherty KT, Burgess P, Tan M, Gasal E, Voi M, Schadendorf D, Long GV. Five-year outcomes with Dabrafenib plus Trametinib in metastatic melanoma. N Engl J Med. 2019;381(7):626–636. doi: 10.1056/NEJMoa1904059. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
