

Countries with delayed COVID-19 introduction - characteristics, drivers, gaps, and opportunities
- PMID: 33731178
- PMCID: PMC7968140
- DOI: 10.1186/s12992-021-00678-4
Countries with delayed COVID-19 introduction - characteristics, drivers, gaps, and opportunities
Abstract
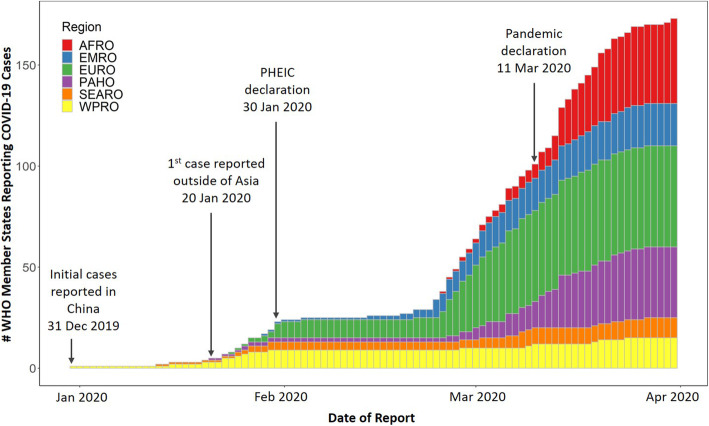
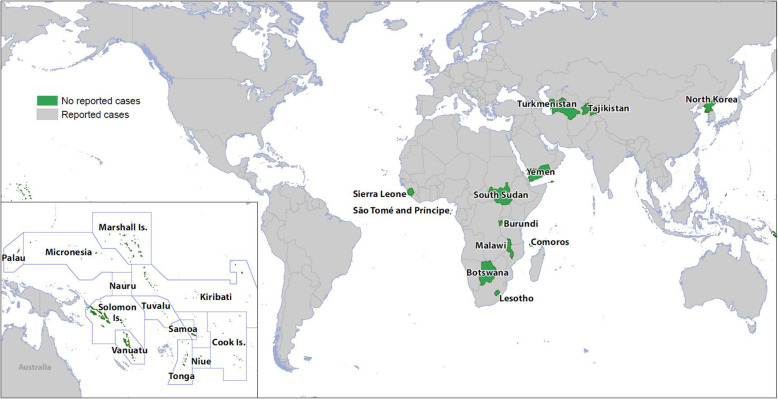
Background: Three months after the first reported cases, COVID-19 had spread to nearly 90% of World Health Organization (WHO) member states and only 24 countries had not reported cases as of 30 March 2020. This analysis aimed to 1) assess characteristics, capability to detect and monitor COVID-19, and disease control measures in these 24 countries, 2) understand potential factors for the reported delayed COVID-19 introduction, and 3) identify gaps and opportunities for outbreak preparedness, particularly in low and middle-income countries (LMICs). We collected and analyzed publicly available information on country characteristics, COVID-19 testing, influenza surveillance, border measures, and preparedness activities in these countries. We also assessed the association between the temporal spread of COVID-19 in all countries with reported cases with globalization indicator and geographic location.
Results: Temporal spreading of COVID-19 was strongly associated with countries' globalization indicator and geographic location. Most of the 24 countries with delayed COVID-19 introduction were LMICs; 88% were small island or landlocked developing countries. As of 30 March 2020, only 38% of these countries reported in-country COVID-19 testing capability, and 71% reported conducting influenza surveillance during the past year. All had implemented two or more border measures, (e.g., travel restrictions and border closures) and multiple preparedness activities (e.g., national preparedness plans and school closing).
Conclusions: Limited testing capacity suggests that most of the 24 delayed countries may have lacked the capability to detect and identify cases early through sentinel and case-based surveillance. Low global connectedness, geographic isolation, and border measures were common among these countries and may have contributed to the delayed introduction of COVID-19 into these countries. This paper contributes to identifying opportunities for pandemic preparedness, such as increasing disease detection, surveillance, and international collaborations. As the global situation continues to evolve, it is essential for countries to improve and prioritize their capacities to rapidly prevent, detect, and respond, not only for COVID-19, but also for future outbreaks.
Keywords: Border control measures; COVID-19; Global health; Pandemic; Preparedness; Surveillance.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- WHO. Novel Coronavirus (2019-nCoV) situation report-1. Geneva: World Health Organization; 2020. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/2.... Accessed 21 Apr 2020.
-
- WHO. Novel Coronavirus (2019-nCoV) situation report-1. Geneva: World Health Organization; 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio.... Accessed 21 Apr 2020.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
