

Current evidence for COVID-19 therapies: a systematic literature review
- PMID: 33731328
- PMCID: PMC9489065
- DOI: 10.1183/16000617.0384-2020
Current evidence for COVID-19 therapies: a systematic literature review
Abstract
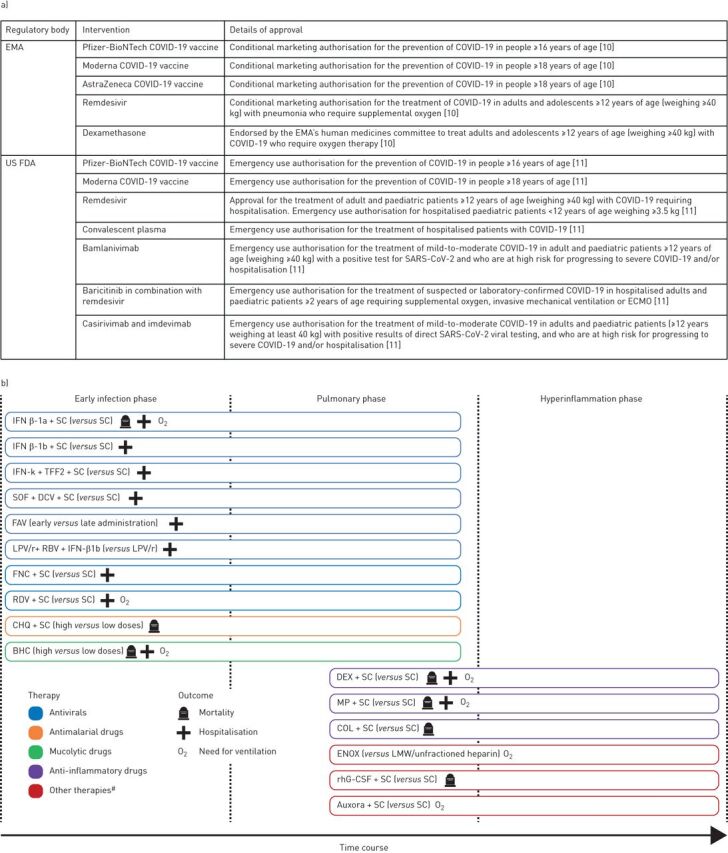
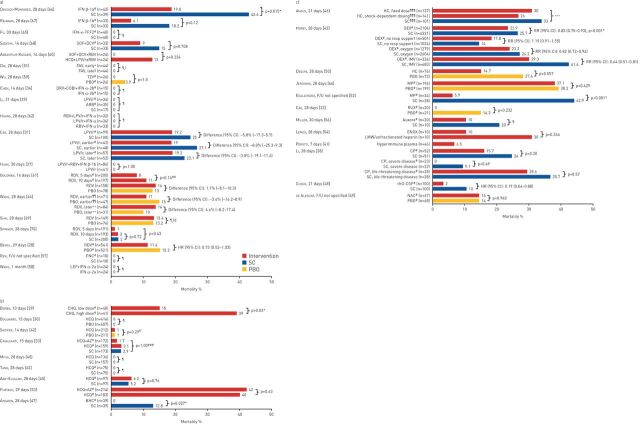
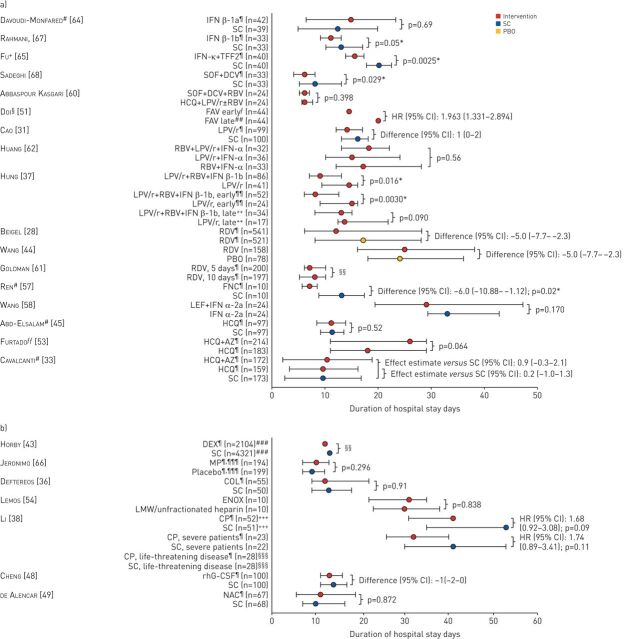
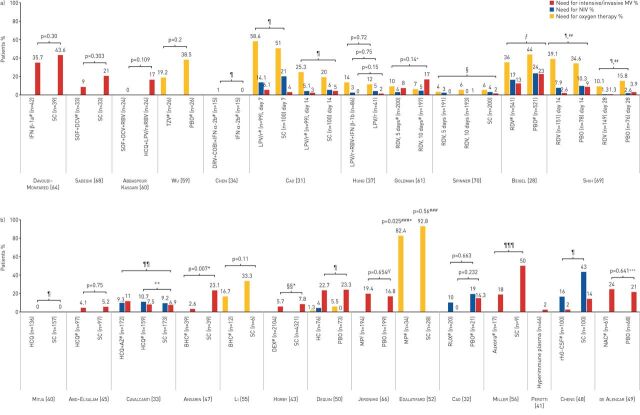
Effective therapeutic interventions for the treatment and prevention of coronavirus disease 2019 (COVID-19) are urgently needed. A systematic review was conducted to identify clinical trials of pharmacological interventions for COVID-19 published between 1 December 2019 and 14 October 2020. Data regarding efficacy of interventions, in terms of mortality, hospitalisation and need for ventilation, were extracted from identified studies and synthesised qualitatively. In total, 42 clinical trials were included. Interventions assessed included antiviral, mucolytic, antimalarial, anti-inflammatory and immunomodulatory therapies. Some reductions in mortality, hospitalisation and need for ventilation were seen with interferons and remdesivir, particularly when administered early, and with the mucolytic drug, bromhexine. Most studies of lopinavir/ritonavir and hydroxychloroquine did not show significant efficacy over standard care/placebo. Dexamethasone significantly reduced mortality, hospitalisation and need for ventilation versus standard care, particularly in patients with severe disease. Evidence for other classes of interventions was limited. Many trials had a moderate-to-high risk of bias, particularly in terms of blinding; most were short-term and some included low patient numbers.This review highlights the need for well-designed clinical trials of therapeutic interventions for COVID-19 to increase the quality of available evidence. It also emphasises the importance of tailoring interventions to disease stage and severity for maximum efficacy.
Copyright ©The authors 2021.
Conflict of interest statement
Conflict of interest: T. Welte reports personal fees, fees for lectures and consultancy fees from AstraZeneca, Basilea, Biotest, Bayer, Boehringer, GlaxoSmithKline, Janssens, Merck Sharp & Dohme, Novartis, Pfizer, Roche and Sanofi Aventis, outside the submitted work. Conflict of interest: L.J. Ambrose reports other funding from AstraZeneca, during the conduct of the study. Conflict of interest: G.C. Sibbring reports other funding from AstraZeneca, during the conduct of the study. Conflict of interest: S. Sheikh was an employee and shareholder of AstraZeneca at the time of manuscript preparation. Conflict of interest: H. Müllerová is an employee and shareholder of AstraZeneca. Conflict of interest: I. Sabir is an employee and shareholder of AstraZeneca.
Figures
References
-
- Institute for Health Metrics and Evaluation . COVID-19 projections. https://covid19.healthdata.org/global?view=total-deaths&tab=trend Date last accessed: 28 January 2021.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources