

Optimizing Oral Medication Schedules for Inpatient Sleep: A Quality Improvement Intervention
- PMID: 33731336
- PMCID: PMC8006200
- DOI: 10.1542/hpeds.2020-002261
Optimizing Oral Medication Schedules for Inpatient Sleep: A Quality Improvement Intervention
Abstract
Objectives: Hospitalized children experience frequent nighttime awakenings. Oral medications are commonly administered around the clock despite the comparable efficacy of daytime administration schedules, which promote sleep. With this study, we evaluated the effectiveness of a quality improvement initiative to increase the proportion of sleep-friendly antibiotic administration schedules.
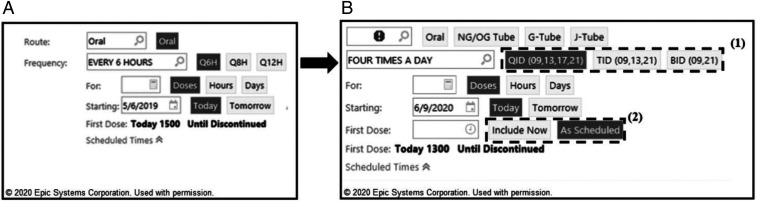
Methods: Interprofessional stakeholders modified computerized provider order entry defaults for 4 oral antibiotic medications, from around the clock to administration occurring exclusively during waking hours. Additionally, care-team members received targeted education. Outcome measures included the proportion of sleep-friendly administration schedules and patient caregiver-reported disruptions to sleep. Pre- and posteducation surveys were used to evaluate education effectiveness. Balancing measures were missed antibiotic doses and related escalations of care.
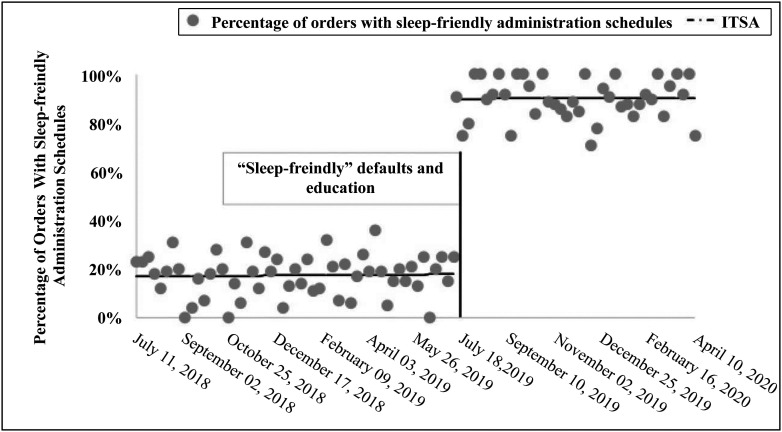
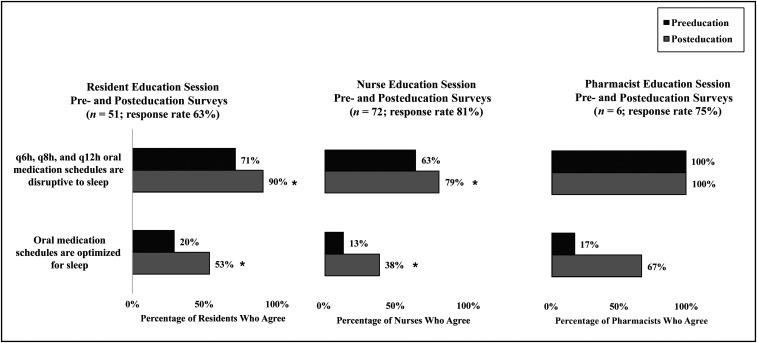
Results: Interrupted time series analysis revealed a 72% increase (interceptpre: 18%; interceptpost: 90%; 95% confidence interval: 65%-79%; P < .001) in intercept for percentage of orders with sleep-friendly administration schedules (orders: n pre = 1014 and n post = 649). Compared with preeducation surveys, care-team members posteducation were more likely to agree that oral medications scheduled around the clock cause sleep disruption (resident: 71% pre, 90% post [P = .01]; nurse: 63% pre, 79% post [P = .03]). Although sleep-friendly orders increased, patient caregivers reported an increase in sleep disruption due to medications (pre 28%, post 46%; P < .001).
Conclusions: A simple, low-cost intervention of computerized provider order entry default modifications and education can increase the proportion of sleep-friendly oral antibiotic administration schedules for hospitalized children. Patient perception of sleep is impacted by multiple factors and often does not align with objective data. An increased focus on improving sleep during hospitalization may result in heightened awareness of disruptions.
Copyright © 2021 by the American Academy of Pediatrics.
Conflict of interest statement
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Nudging towards Sleep-Friendly Health Care: A Multifaceted Approach on Reducing Unnecessary Overnight Interventions.Appl Clin Inform. 2024 Oct;15(5):1025-1039. doi: 10.1055/a-2404-2344. Epub 2024 Aug 27. Appl Clin Inform. 2024. PMID: 39191425 Free PMC article.
-
Improving Hospitalized Children's Sleep by Reducing Excessive Overnight Blood Pressure Monitoring.Pediatrics. 2020 Sep;146(3):e20192217. doi: 10.1542/peds.2019-2217. Pediatrics. 2020. PMID: 32817268 Free PMC article.
-
Perspective: leveraging the electronic health record to improve sleep in the hospital.J Clin Sleep Med. 2023 Feb 1;19(2):421-423. doi: 10.5664/jcsm.10360. J Clin Sleep Med. 2023. PMID: 36448329 Free PMC article.
-
Caregiver and Staff Perceptions of Disruptions to Pediatric Inpatient Sleep.J Clin Sleep Med. 2018 Nov 15;14(11):1895-1902. doi: 10.5664/jcsm.7488. J Clin Sleep Med. 2018. PMID: 30373684 Free PMC article.
-
Clinical Practice Guideline: Tonsillectomy in Children (Update)-Executive Summary.Otolaryngol Head Neck Surg. 2019 Feb;160(2):187-205. doi: 10.1177/0194599818807917. Otolaryngol Head Neck Surg. 2019. PMID: 30921525 Review.
Cited by
-
How to Improve the Sleep of Hospitalized Pediatric Patients: Family and Staff Focus Groups.Transplant Cell Ther. 2025 Aug;31(8):586.e1-586.e11. doi: 10.1016/j.jtct.2025.05.025. Epub 2025 Jun 7. Transplant Cell Ther. 2025. PMID: 40490080
-
Sleep in hospitalized pediatric and adult patients - A systematic review and meta-analysis.Sleep Med X. 2022 Nov 5;4:100059. doi: 10.1016/j.sleepx.2022.100059. eCollection 2022 Dec. Sleep Med X. 2022. PMID: 36406659 Free PMC article.
-
Describing the evidence linking interprofessional education interventions to improving the delivery of safe and effective patient care: a scoping review.J Interprof Care. 2024 May-Jun;38(3):476-485. doi: 10.1080/13561820.2023.2283119. Epub 2023 Dec 20. J Interprof Care. 2024. PMID: 38124506 Free PMC article.
-
Nudging towards Sleep-Friendly Health Care: A Multifaceted Approach on Reducing Unnecessary Overnight Interventions.Appl Clin Inform. 2024 Oct;15(5):1025-1039. doi: 10.1055/a-2404-2344. Epub 2024 Aug 27. Appl Clin Inform. 2024. PMID: 39191425 Free PMC article.
-
Use of machine learning to identify risk factors for insomnia.PLoS One. 2023 Apr 12;18(4):e0282622. doi: 10.1371/journal.pone.0282622. eCollection 2023. PLoS One. 2023. PMID: 37043435 Free PMC article.
References
-
- American Board of Internal Medicine Choosing Wisely Initiative. American Academy of Nursing: don’t wake patients for routine care choosing wisely. 2014. Available at: http://www.choosingwisely.org/clinician-lists/american-academy-nursing-a.... Accessed June 14, 2019
-
- Stremler R, Adams S, Dryden-Palmer K. Nurses’ views of factors affecting sleep for hospitalized children and their families: a focus group study. Res Nurs Health. 2015;38(4):311–322 - PubMed
-
- Herbert AR, de Lima J, Fitzgerald DA, Seton C, Waters KA, Collins JJ. Exploratory study of sleeping patterns in children admitted to hospital. J Paediatr Child Health. 2014;50(8):632–638 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
