

Association of HLA Class I Genotypes With Severity of Coronavirus Disease-19
- PMID: 33732261
- PMCID: PMC7959787
- DOI: 10.3389/fimmu.2021.641900
Association of HLA Class I Genotypes With Severity of Coronavirus Disease-19
Abstract
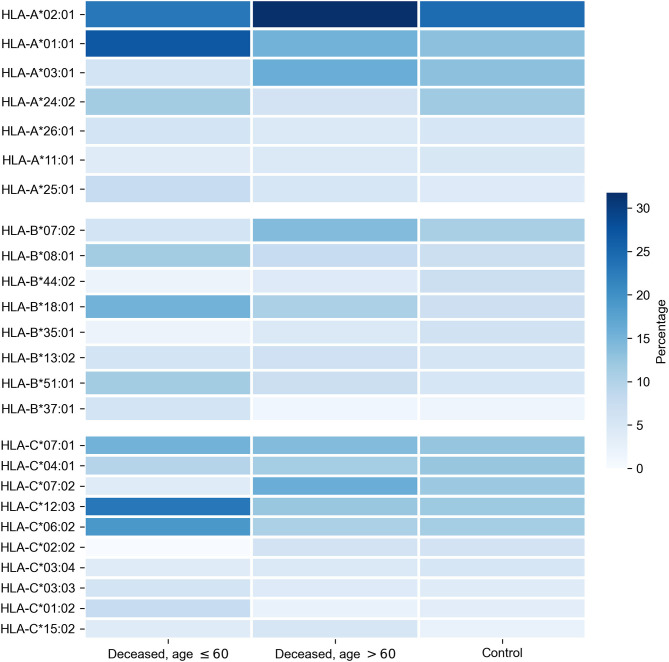
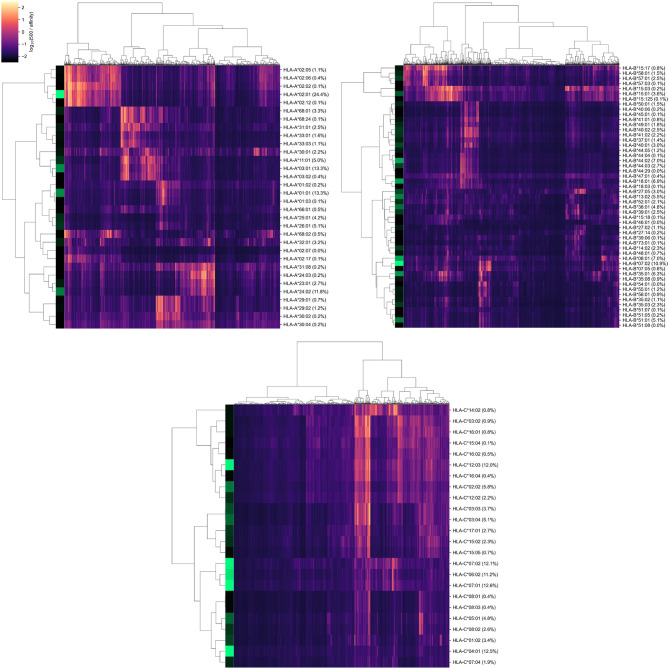
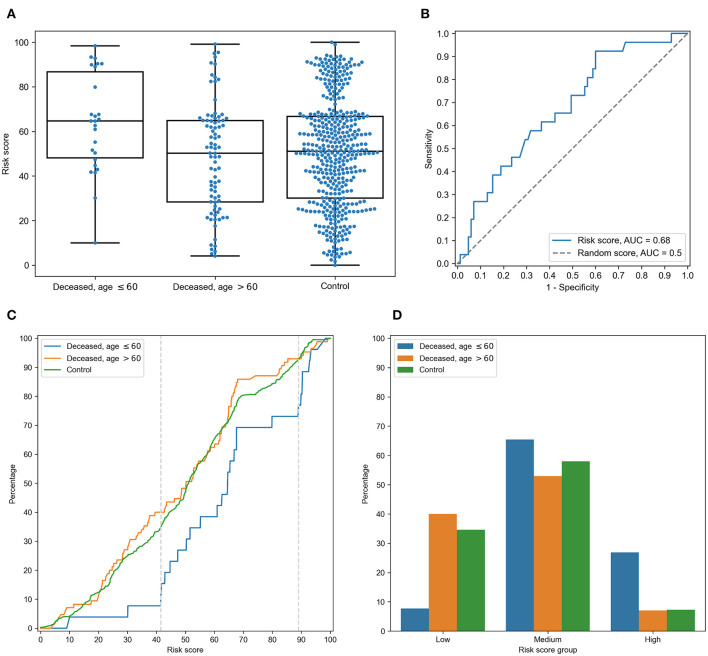
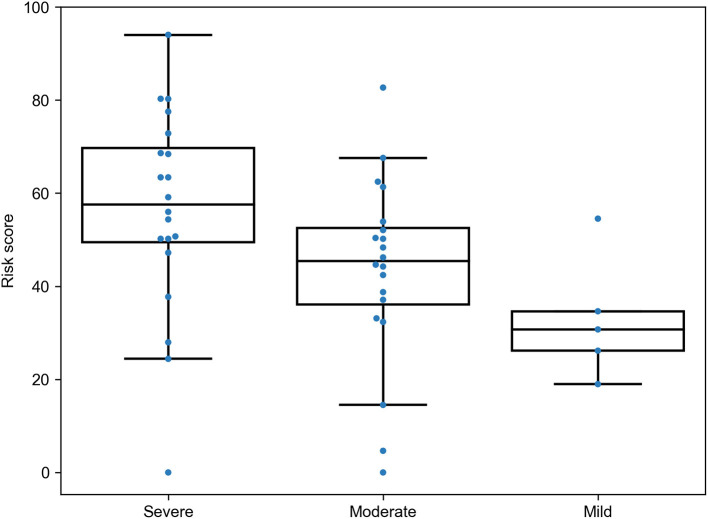
Human leukocyte antigen (HLA) class I molecules play a crucial role in the development of a specific immune response to viral infections by presenting viral peptides at the cell surface where they will be further recognized by T cells. In the present manuscript, we explored whether HLA class I genotypes can be associated with the critical course of Coronavirus Disease-19 by searching possible connections between genotypes of deceased patients and their age at death. HLA-A, HLA-B, and HLA-C genotypes of n = 111 deceased patients with COVID-19 (Moscow, Russia) and n = 428 volunteers were identified with next-generation sequencing. Deceased patients were split into two groups according to age at the time of death: n = 26 adult patients aged below 60 and n = 85 elderly patients over 60. With the use of HLA class I genotypes, we developed a risk score (RS) which was associated with the ability to present severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) peptides by the HLA class I molecule set of an individual. The resulting RS was significantly higher in the group of deceased adults compared to elderly adults [p = 0.00348, area under the receiver operating characteristic curve (AUC ROC = 0.68)]. In particular, presence of HLA-A*01:01 allele was associated with high risk, while HLA-A*02:01 and HLA-A*03:01 mainly contributed to low risk. The analysis of patients with homozygosity strongly highlighted these results: homozygosity by HLA-A*01:01 accompanied early deaths, while only one HLA-A*02:01 homozygote died before 60 years of age. Application of the constructed RS model to an independent Spanish patients cohort (n = 45) revealed that the score was also associated with the severity of the disease. The obtained results suggest the important role of HLA class I peptide presentation in the development of a specific immune response to COVID-19.
Keywords: COVID-19; HLA class I; MHC class I; SARS-CoV-2; peptide presentation.
Copyright © 2021 Shkurnikov, Nersisyan, Jankevic, Galatenko, Gordeev, Vechorko and Tonevitsky.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous