

Cost-effectiveness of Remdesivir and Dexamethasone for COVID-19 Treatment in South Africa
- PMID: 33732750
- PMCID: PMC7928624
- DOI: 10.1093/ofid/ofab040
Cost-effectiveness of Remdesivir and Dexamethasone for COVID-19 Treatment in South Africa
Abstract
Background: Dexamethasone and remdesivir have the potential to reduce coronavirus disease 2019 (COVID)-related mortality or recovery time, but their cost-effectiveness in countries with limited intensive care resources is unknown.
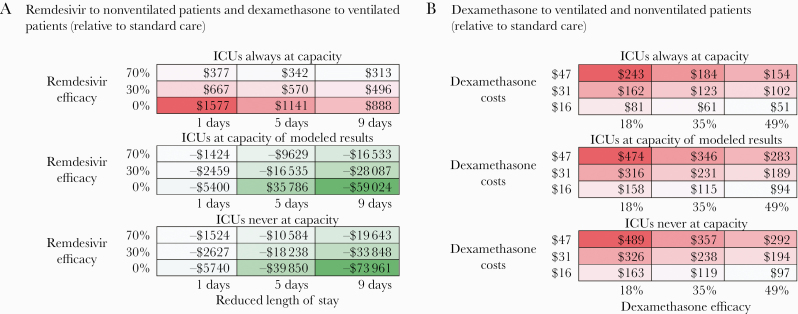
Methods: We projected intensive care unit (ICU) needs and capacity from August 2020 to January 2021 using the South African National COVID-19 Epi Model. We assessed the cost-effectiveness of (1) administration of dexamethasone to ventilated patients and remdesivir to nonventilated patients, (2) dexamethasone alone to both nonventilated and ventilated patients, (3) remdesivir to nonventilated patients only, and (4) dexamethasone to ventilated patients only, all relative to a scenario of standard care. We estimated costs from the health care system perspective in 2020 US dollars, deaths averted, and the incremental cost-effectiveness ratios of each scenario.
Results: Remdesivir for nonventilated patients and dexamethasone for ventilated patients was estimated to result in 408 (uncertainty range, 229-1891) deaths averted (assuming no efficacy [uncertainty range, 0%-70%] of remdesivir) compared with standard care and to save $15 million. This result was driven by the efficacy of dexamethasone and the reduction of ICU-time required for patients treated with remdesivir. The scenario of dexamethasone alone for nonventilated and ventilated patients requires an additional $159 000 and averts 689 [uncertainty range, 330-1118] deaths, resulting in $231 per death averted, relative to standard care.
Conclusions: The use of remdesivir for nonventilated patients and dexamethasone for ventilated patients is likely to be cost-saving compared with standard care by reducing ICU days. Further efforts to improve recovery time with remdesivir and dexamethasone in ICUs could save lives and costs in South Africa.
Keywords: COVID-19; SARS-CoV-2; cost-effectiveness; dexamethasone; hospital bed capacity; intensive care; mathematical model; remdesivir.
© The Author(s) 2021. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures

Update of
-
Cost-effectiveness of remdesivir and dexamethasone for COVID-19 treatment in South Africa.medRxiv [Preprint]. 2020 Sep 27:2020.09.24.20200196. doi: 10.1101/2020.09.24.20200196. medRxiv. 2020. Update in: Open Forum Infect Dis. 2021 Jan 29;8(3):ofab040. doi: 10.1093/ofid/ofab040. PMID: 32995824 Free PMC article. Updated. Preprint.
References
-
- Roser M, Ritchie H, Ortiz-Ospina E, Hasell J. Coronavirus pandemic (COVID-19). 2020. Available at: https://ourworldindata.org/coronavirus. Accessed 6 June 2020.
-
- Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). COVID-19 dashboard. Available at: https://coronavirus.jhu.edu/map.html. Accessed 20 July 2020.
-
- Magome M. Oxygen already runs low as COVID-19 surges in South Africa. The Washington Post. 10 July 2020. Available at: https://www.washingtonpost.com/world/africa/oxygen-already-runs-low-as-c.... Accessed 10 July 2020.
-
- Kim L, Garg S, O’Halloran A, et al. Risk factors for intensive care unit admission and in-hospital mortality among hospitalized adults identified through the U.S. coronavirus disease 2019 (COVID-19)-associated hospitalization surveillance network (COVID-NET) [published online ahead of print July 16, 2020]. Clin Infect Dis 2020. doi: 10.1093/cid/ciaa1012 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
