

Pooled Analysis of Roxadustat for Anemia in Patients With Kidney Failure Incident to Dialysis
- PMID: 33732976
- PMCID: PMC7938204
- DOI: 10.1016/j.ekir.2020.12.018
Pooled Analysis of Roxadustat for Anemia in Patients With Kidney Failure Incident to Dialysis
Retraction in
-
Retraction notice to "Pooled Analysis of Roxadustat for Anemia in Patients With Kidney Failure Incident to Dialysis." Kidney Int Rep. 2021;6:613-623.Kidney Int Rep. 2022 Feb 5;7(3):665. doi: 10.1016/j.ekir.2022.01.1069. eCollection 2022 Mar. Kidney Int Rep. 2022. PMID: 35257087 Free PMC article.
Abstract
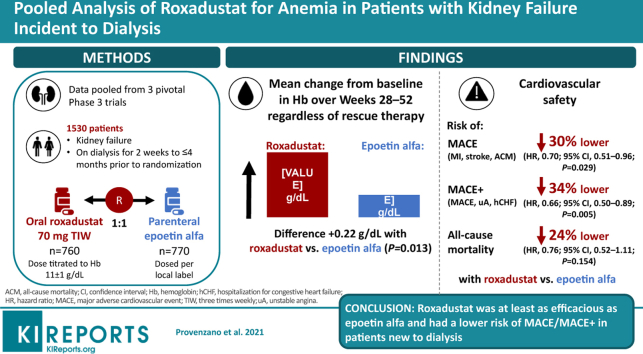
Introduction: Erythropoiesis-stimulating agents are associated with increased cardiovascular risk when higher doses are used toward higher hematocrit targets. Patients new to dialysis are at higher risk for morbidity and mortality. Systematic evaluation of this population was predefined in the roxadustat clinical development program. Roxadustat is a hypoxia-inducible prolyl hydroxylase inhibitor.
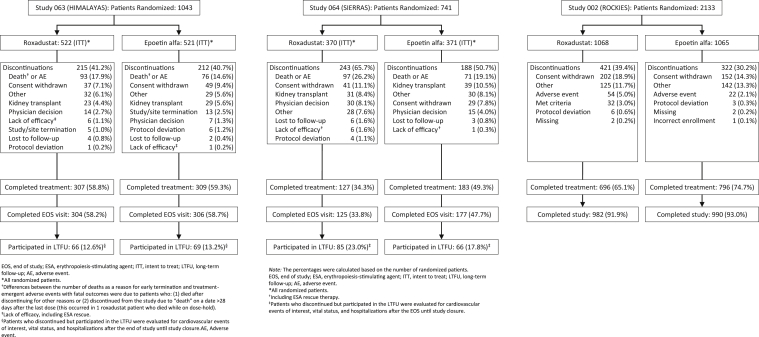
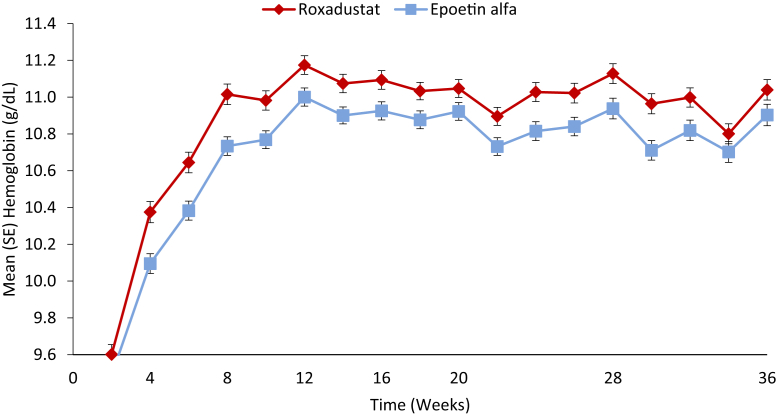
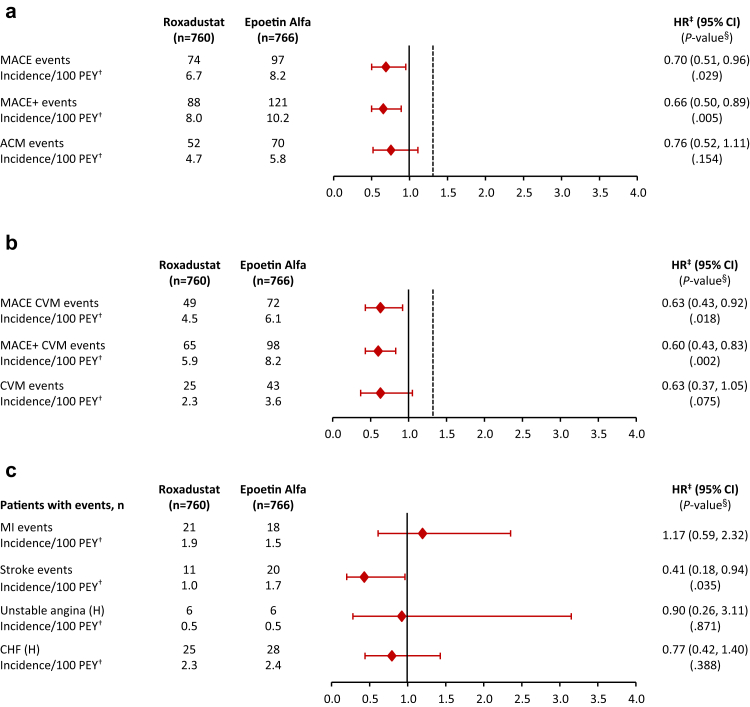
Methods: Data were pooled from 3 phase 3, randomized, open-label, active-controlled trials. Eligible adults had kidney failure and initiated dialysis for 2 weeks to ≤ 4 months prior to randomization to roxadustat or epoetin alfa. Efficacy was assessed as mean change in hemoglobin from baseline averaged over weeks 28 to 52, regardless of rescue therapy. Key cardiovascular safety endpoints were major adverse cardiovascular events (MACE; all-cause mortality [ACM], myocardial infarction, and stroke), and MACE+ (MACE plus unstable angina or congestive heart failure requiring hospitalization), and ACM.
Results: This study included 1530 patients with kidney failure incident to dialysis. Mean (SD) changes in hemoglobin from baseline averaged over weeks 28 to 52, regardless of rescue therapy, were 2.12 (1.45) versus 1.91 (1.42) g/dl in the roxadustat and epoetin alfa groups (least-squares mean difference: 0.22; 95% CI, 0.05 to 0.40; P = 0.0130). Risks of MACE and MACE+ were lower in the roxadustat group (hazard ratio [HR], 0.70; 95% CI, 0.51 to 0.96) than the epoetin alfa group (HR, 0.66; 95% CI, 0.50 to 0.89); the HR for ACM was 0.76 (95% CI, 0.52 to 1.11).
Conclusion: Roxadustat was at least as efficacious as epoetin alfa. Roxadustat had a lower risk of MACE/MACE+ in patients new to dialysis.
Keywords: anemia; chronic kidney disease; dialysis; roxadustat.
© 2020 International Society of Nephrology. Published by Elsevier Inc.
Figures

Comment in
-
Roxadustat for CKD Anemia - Starting the Jigsaw Puzzle, What Will the Finished Picture Show?Kidney Int Rep. 2021 Feb 4;6(3):559-561. doi: 10.1016/j.ekir.2021.01.035. eCollection 2021 Mar. Kidney Int Rep. 2021. Retraction in: Kidney Int Rep. 2022 Feb 05;7(3):665. doi: 10.1016/j.ekir.2022.01.1070. PMID: 33735328 Free PMC article. Retracted. No abstract available.
References
-
- Couser W.G., Remuzzi G., Mendis S. The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int. 2011;80:1258–1270. - PubMed
-
- United States Renal Data System . National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda, MD: 2018. Chapter 1. Incidence, prevalence, patient characteristics, and treatment modalities.
-
- Eggers P.W. Mortality rates among dialysis patients in Medicare's End-Stage Renal Disease Program. Am J Kidney Dis. 1990;15:414–421. - PubMed
-
- United States Renal Data System . National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda, MD: 2007. Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States.
-
- Foley R.N., Chen S.C., Solid C.A. Early mortality in patients starting dialysis appears to go unregistered. Kidney Int. 2014;86:392–398. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
