

Kidney Involvement in Patients With Chronic Myelomonocytic Leukemia or BCR-ABL-Negative Myeloproliferative Neoplasms
- PMID: 33732988
- PMCID: PMC7938079
- DOI: 10.1016/j.ekir.2020.12.005
Kidney Involvement in Patients With Chronic Myelomonocytic Leukemia or BCR-ABL-Negative Myeloproliferative Neoplasms
Abstract
Introduction: The identification of specific molecular signatures and the development of new targeted drugs have changed the paradigm of onco-nephrology, now allowing a multiscale approach of kidney involvement related to hematologic malignancies relying on combined hematologic and molecular assessments. In this study, we aimed to refine the spectrum of kidney disorders associated with chronic myelomonocytic leukemia (CMML) or BCR-ABL-negative myeloproliferative neoplasms (MPNs), 2 very rare conditions scarcely described.
Methods: Case series. Patients with myeloid neoplasms who were referred to Toulouse University Hospital Nephrology Unit and were diagnosed with acute kidney injury (AKI), chronic kidney disease (CKD), or urine abnormalities were retrospectively included.
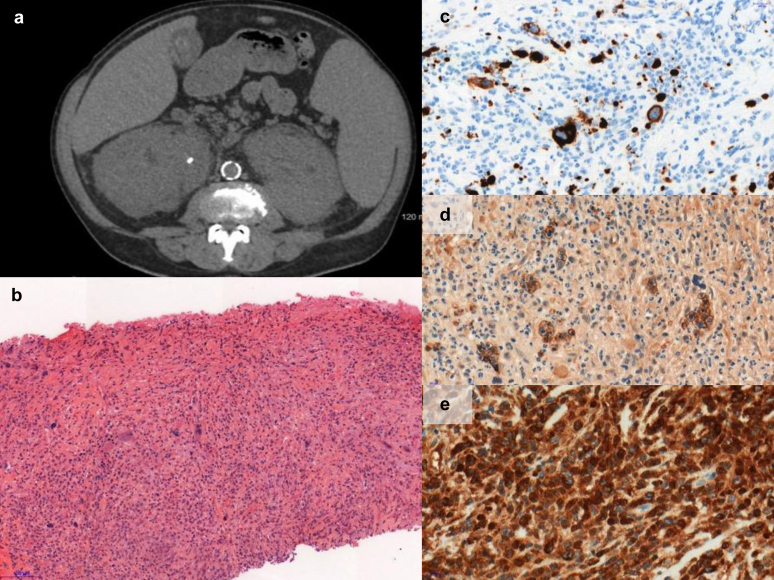
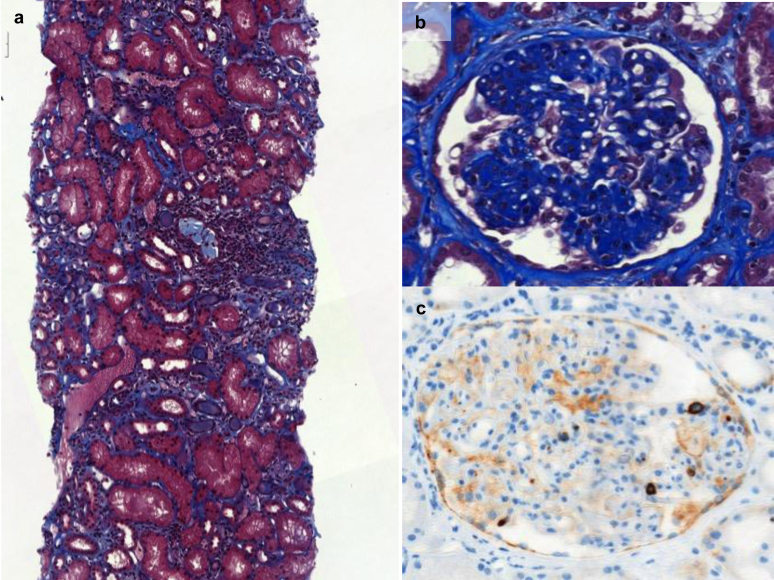
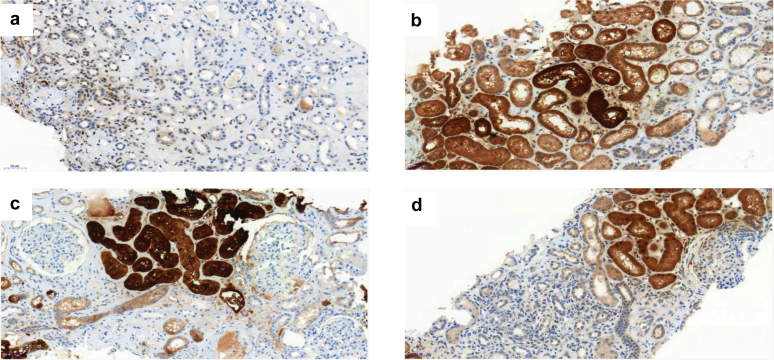
Results: Eighteen patients (males n=13, CMML n=8, essential thrombocytosis [ET] n=7, polycythemia vera [PV] n=1, and myelofibrosis n=2) developed kidney disease 7.7±2 years after the diagnosis of the malignancy. Twelve patients had AKI at presentation. Eight patients had glomerular presentation (high-range proteinuria 33%, microscopic hematuria 56%). Kidney biopsy (n=14) showed various patterns, including pauci-immune glomerulosclerosis (n=5), extramedullary hematopoiesis (n=6), or tubular atrophy and interstitial fibrosis with polymorphic inflammation (n=8). Immunostaining of CD61 confirmed the infiltration of megakaryocytes within glomeruli or interstitium in 5 of 8 patients. Other pictures of glomerulopathy were identified in 3 patients (IgA nephropathy n=2, AA amyloidosis n=1). Massive kidney infiltration by CMML was identified in 1 patient. After a mean follow-up of 24±6 months, malignancy was considered as stable in 11 patients (61%), but 22% of patients had progressed to end-stage renal failure. The remaining had persistently reduced kidney function. No correlation between the malignancy and the renal presentation and outcomes could be identified.
Conclusions: Kidney complications of CMML/MPN are heterogenous, and kidney biopsy may help to identify new molecular targets to prevent the development of kidney fibrosis.
Keywords: chronic kidney disease; chronic myelomonocytic leukemia; essential thrombocytosis; megakaryocytes; myeloid neoplasms; myeloproliferative neoplasms.
© 2021 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
-
- Arber D.A., Orazi A., Hasserjian R. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127:2391–2405. - PubMed
-
- Skoda R.C., Duek A., Grisouard J. Pathogenesis of myeloproliferative neoplasms. Exp Hematol. 2015;43:599–608. - PubMed
-
- Zimran E., Hoffman R., Kremyanskaya M. Current approaches to challenging scenarios in myeloproliferative neoplasms. Expert Rev Anticancer Ther. 2018;18:567–578. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
