

Provoked versus unprovoked venous thromboembolism: Findings from GARFIELD-VTE
- PMID: 33733032
- PMCID: PMC7938631
- DOI: 10.1002/rth2.12482
Provoked versus unprovoked venous thromboembolism: Findings from GARFIELD-VTE
Abstract
Introduction: Venous thromboembolism (VTE) has a long-term risk of recurrence, dependent on the presence or absence of provoking risk factors at the time of the event.
Objective: To compare clinical characteristics, anticoagulant patterns, and 12-month outcomes in patients with transient provoking factors, active cancer, and unprovoked VTE.
Methods: The Global Anticoagulant Registry in the FIELD (GARFIELD)-VTE is a prospective, observational study that enrolled 10 207 patients with objectively diagnosed VTE from 415 sites in 28 countries.
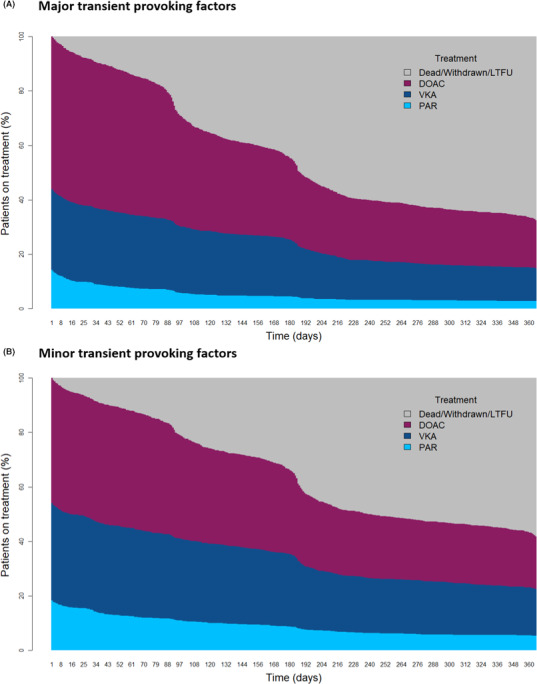
Results: Patients with transient provoking factors were younger (53.0 years) and more frequently women (61.2%) than patients with unprovoked VTE (60.3 years; 43.0% women) or active cancer (63.6 years; 51.7% women). After 6 months, 59.1% of patients with transient provoking factors remained on anticoagulation, compared to 71.3% with unprovoked VTE and 47.3% with active cancer. At 12 months, this decreased to 36.7%, 51.5%, and 25.4%, respectively. The risk of mortality (hazard ratio [HR], 1.21; 95% confidence interval [CI], 0.90-1.62), recurrent VTE (HR, 0.84; 95% CI, 0.62-1.14), and major bleeding (HR, 1.26; 95% CI, 0.86-1.85) was comparable in patients with transient provoking factors and unprovoked VTE. Patients with minor and major transient provoking factors had a similar risk of recurrent VTE (HR, 0.99; 95% CI, 0.59-1.66), but those with major transient risk factors had a lower risk of death (HR, 0.61; 95% CI, 0.38-0.98).
Conclusion: At 1 year, nearly 40% of patients with transient provoking factors and slightly over half of patients with unprovoked VTE were on anticoagulant treatment. Event rates were comparable between the two groups. Risk of death was higher in patients with minor transient factors than in those with major transient factors.
Keywords: anticoagulants; deep vein thrombosis; pulmonary embolism; risk factors; venous thromboembolism.
© 2021 The Authors. Research and Practice in Thrombosis and Haemostasis published by Wiley Periodicals LLC on behalf of International Society on Thrombosis and Haemostasis (ISTH).
Figures





References
-
- Hutten BA, Prins MH, Gent M, Ginsberg J, Tijssen JGP, Büller HR, et al. Incidence of recurrent thromboembolic and bleeding complications among patients with venous thromboembolism in relation to both malignancy and achieved international normalized ratio: a retrospective analysis. J Clin Oncol. 2000;18(17):3078–83. - PubMed
-
- Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence‐Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e419S–e496S. - PMC - PubMed
-
- Tromeur C, Sanchez O, Presles E, Pernod G, Bertoletti L, Jego P, et al. Risk factors for recurrent venous thromboembolism after unprovoked pulmonary embolism: the PADIS‐PE randomised trial. Eur Respir J. 2018;51(1):1701202. - PubMed
-
- Iorio A, Kearon C, Filippucci E, Marcucci M, Macura A, Pengo V, et al. Risk of recurrence after a first episode of symptomatic venous thromboembolism provoked by a transient risk factor: a systematic review. Arch Intern Med. 2010;170(19):1710–6. - PubMed
-
- Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing G‐J, Harjola V‐P, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS): The Task Force for the diagnosis and management of acute pulmonary embolism of the European Society of Cardiology (ESC). Eur Respir J. 2019;54(3):1901647. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
