

Reliability of respiratory-triggered two-dimensional cine k-adaptive-t-autocalibrating reconstruction for Cartesian sampling for the assessment of biventricular volume and function in patients with repaired tetralogy of Fallot
- PMID: 33733811
- PMCID: PMC8010533
- DOI: 10.1259/bjr.20201249
Reliability of respiratory-triggered two-dimensional cine k-adaptive-t-autocalibrating reconstruction for Cartesian sampling for the assessment of biventricular volume and function in patients with repaired tetralogy of Fallot
Abstract
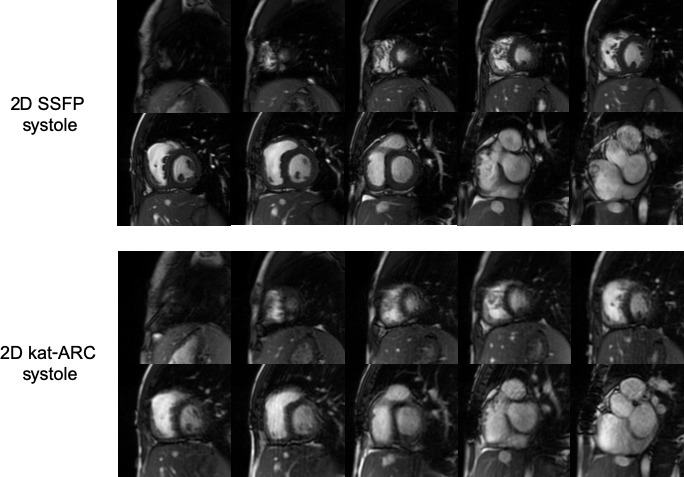
Objective: To compare left ventricular (LV) and right ventricular (RV) volume, function, and image quality of a respiratory-triggered two-dimensional (2D)-cine k-adaptive-t-autocalibrating reconstruction for Cartesian sampling (2D kat-ARC) with those of the standard reference, namely, breath-hold 2D balanced steady-state free precession (2D SSFP), in patients with repaired tetralogy of Fallot (TOF).
Methods: 30 patients (14 males, mean age 32.2 ± 13.9 years) underwent cardiac magnetic resonance, and 2D kat-ARC and 2D SSFP images were acquired on short-axis view. Biventricular end-diastolic volume (EDV) and end-systolic volume (ESV), stroke volume (SV), ejection fraction (EF), and LV mass (LVM) were analysed.
Results: The 2D kat-ARC had significantly shorter scan time (35.2 ± 9.1 s vs 80.4 ± 16.7 s; p < 0.0001). Despite an analysis of image quality showed significant impairment using 2D kat-ARC compared to 2D SSFP cine (p < 0.0001), the two sequences demonstrated no significant difference in terms of biventricular EDV, LVESV, LVSV, LVEF, and LVM. However, the RVESV was overestimated for 2D kat-ARC compared with that for 2D SSFP (73.8 ± 43.2 ml vs 70.3 ± 44.5 ml, p = 0.0002) and the RVSV and RVEF were underestimated (RVSV = 46.2±20.5 ml vs 49.4 ± 20.4 ml, p = 0.0024; RVEF = 40.2±12.7% vs. 43.5±14.0%, p = 0.0002).
Conclusion: Respiratory-triggered 2D kat-ARC cine is a reliable technique that could be used in the evaluation of LV volumes and function.
Advances in knowledge: 2D cine kat-ARC is a reliable technique for the assessment LV volume and function in patients with repaired TOF.
Figures



Similar articles
-
Reliability of respiratory-gated real-time two-dimensional cine incorporating deep learning reconstruction for the assessment of ventricular function in an adult population.Int J Cardiovasc Imaging. 2023 May;39(5):1001-1011. doi: 10.1007/s10554-023-02793-2. Epub 2023 Jan 17. Int J Cardiovasc Imaging. 2023. PMID: 36648573
-
MRI Assessment of Right Ventricular Volumes and Function in Patients With Repaired Tetralogy of Fallot Using kat-ARC Accelerated Sequences.AJR Am J Roentgenol. 2020 Oct;215(4):807-817. doi: 10.2214/AJR.19.22726. Epub 2020 Aug 5. AJR Am J Roentgenol. 2020. PMID: 32755352
-
Reliability of single breath hold three-dimensional cine kat-ARC for the assessment of biventricular dimensions and function.Eur J Radiol. 2020 Mar;124:108820. doi: 10.1016/j.ejrad.2020.108820. Epub 2020 Jan 8. Eur J Radiol. 2020. PMID: 31951894
-
Feasibility of Three-Dimensional Balanced Steady-State Free Precession Cine Magnetic Resonance Imaging Combined with an Image Denoising Technique to Evaluate Cardiac Function in Children with Repaired Tetralogy of Fallot.Korean J Radiol. 2021 Sep;22(9):1525-1536. doi: 10.3348/kjr.2020.0850. Korean J Radiol. 2021. PMID: 34448382 Free PMC article.
-
Advanced imaging for pre- and post-operative evaluation of tetralogy of Fallot.Clin Imaging. 2025 Apr;120:110432. doi: 10.1016/j.clinimag.2025.110432. Epub 2025 Feb 12. Clin Imaging. 2025. PMID: 39954316 Review.
Cited by
-
Reliability of respiratory-gated real-time two-dimensional cine incorporating deep learning reconstruction for the assessment of ventricular function in an adult population.Int J Cardiovasc Imaging. 2023 May;39(5):1001-1011. doi: 10.1007/s10554-023-02793-2. Epub 2023 Jan 17. Int J Cardiovasc Imaging. 2023. PMID: 36648573
-
Differential subsampling with cartesian ordering: A high spatial-temporal resolution dixon imaging sequence for assessment of dural arteriovenous fistula.Front Neurol. 2022 Oct 18;13:1020749. doi: 10.3389/fneur.2022.1020749. eCollection 2022. Front Neurol. 2022. PMID: 36330430 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
