

Effectiveness of Electroacupuncture or Auricular Acupuncture vs Usual Care for Chronic Musculoskeletal Pain Among Cancer Survivors: The PEACE Randomized Clinical Trial
- PMID: 33734288
- PMCID: PMC7974834
- DOI: 10.1001/jamaoncol.2021.0310
Effectiveness of Electroacupuncture or Auricular Acupuncture vs Usual Care for Chronic Musculoskeletal Pain Among Cancer Survivors: The PEACE Randomized Clinical Trial
Abstract
Importance: The opioid crisis creates challenges for cancer pain management. Acupuncture confers clinical benefits for chronic nonmalignant pain, but its effectiveness in cancer survivors remains uncertain.
Objective: To determine the effectiveness of electroacupuncture or auricular acupuncture for chronic musculoskeletal pain in cancer survivors.
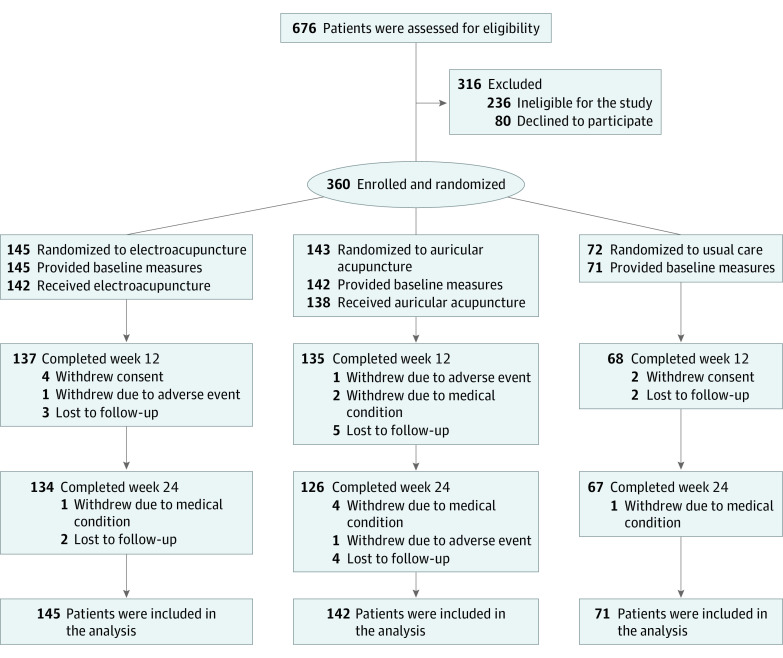
Design, setting, and participants: The Personalized Electroacupuncture vs Auricular Acupuncture Comparative Effectiveness (PEACE) trial is a randomized clinical trial that was conducted from March 2017 to October 2019 (follow-up completed April 2020) across an urban academic cancer center and 5 suburban sites in New York and New Jersey. Study statisticians were blinded to treatment assignments. The 360 adults included in the study had a prior cancer diagnosis but no current evidence of disease, reported musculoskeletal pain for at least 3 months, and self-reported pain intensity on the Brief Pain Inventory (BPI) ranging from 0 (no pain) to 10 (worst pain imaginable).
Interventions: Patients were randomized 2:2:1 to electroacupuncture (n = 145), auricular acupuncture (n = 143), or usual care (n = 72). Intervention groups received 10 weekly sessions of electroacupuncture or auricular acupuncture. Ten acupuncture sessions were offered to the usual care group from weeks 12 through 24.
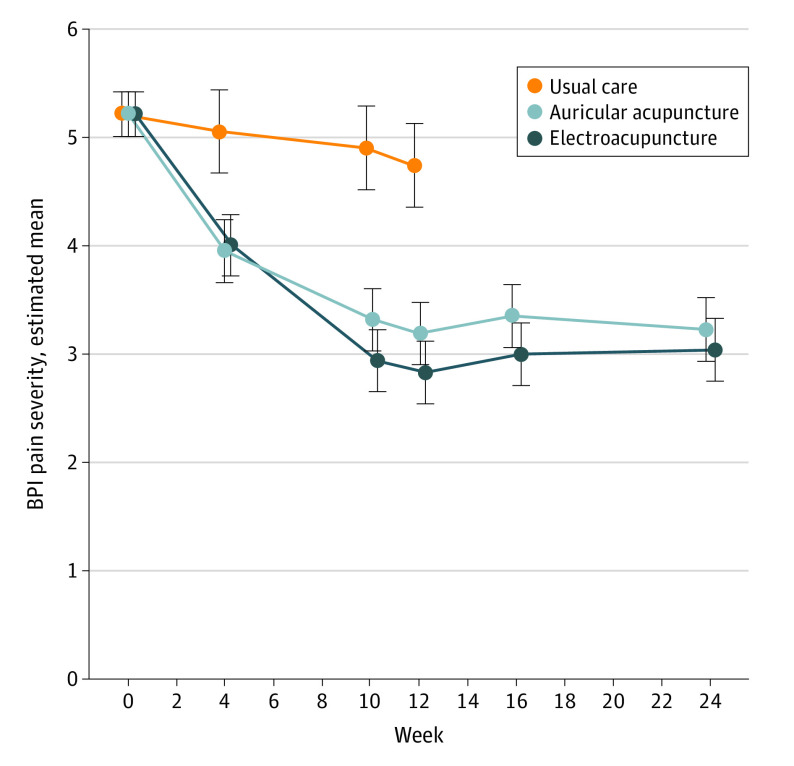
Main outcomes and measures: The primary outcome was change in average pain severity score on the BPI from baseline to week 12. Using a gatekeeping multiple-comparison procedure, electroacupuncture and auricular acupuncture were compared with usual care using a linear mixed model. Noninferiority of auricular acupuncture to electroacupuncture was tested if both interventions were superior to usual care.
Results: Among 360 cancer survivors (mean [SD] age, 62.1 [12.7] years; mean [SD] baseline BPI score, 5.2 [1.7] points; 251 [69.7%] women; and 88 [24.4%] non-White), 340 (94.4%) completed the primary end point. Compared with usual care, electroacupuncture reduced pain severity by 1.9 points (97.5% CI, 1.4-2.4 points; P < .001) and auricular acupuncture reduced by 1.6 points (97.5% CI, 1.0-2.1 points; P < .001) from baseline to week 12. Noninferiority of auricular acupuncture to electroacupuncture was not demonstrated. Adverse events were mild; 15 of 143 (10.5%) patients receiving auricular acupuncture and 1 of 145 (0.7%) patients receiving electroacupuncture discontinued treatments due to adverse events (P < .001).
Conclusions and relevance: In this randomized clinical trial among cancer survivors with chronic musculoskeletal pain, electroacupuncture and auricular acupuncture produced greater pain reduction than usual care. However, auricular acupuncture did not demonstrate noninferiority to electroacupuncture, and patients receiving it had more adverse events.
Trial registration: ClinicalTrials.gov Identifier: NCT02979574.
Conflict of interest statement
Figures
Comment in
-
Acupuncture for Cancer Survivors.JAMA Oncol. 2021 Sep 1;7(9):1399-1400. doi: 10.1001/jamaoncol.2021.2517. JAMA Oncol. 2021. PMID: 34323934 No abstract available.
-
Acupuncture for Cancer Survivors-Reply.JAMA Oncol. 2021 Sep 1;7(9):1400-1401. doi: 10.1001/jamaoncol.2021.2520. JAMA Oncol. 2021. PMID: 34323960 No abstract available.
-
Acupuncture for Cancer Survivors.JAMA Oncol. 2021 Sep 1;7(9):1399. doi: 10.1001/jamaoncol.2021.2514. JAMA Oncol. 2021. PMID: 34323969 No abstract available.
References
-
- Steglitz J, Buscemi J, Ferguson MJ. The future of pain research, education, and treatment: a summary of the IOM report “Relieving pain in America: a blueprint for transforming prevention, care, education, and research”. Transl Behav Med. 2012;2(1):6-8. doi: 10.1007/s13142-012-0110-2 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
