

Transfer of fresh or frozen embryos: a randomised controlled trial
- PMID: 33734369
- PMCID: PMC7970725
- DOI: 10.1093/humrep/deaa305
Transfer of fresh or frozen embryos: a randomised controlled trial
Abstract
Study question: Is IVF with frozen-thawed blastocyst transfer (freeze-all strategy) more effective than IVF with fresh and frozen-thawed blastocyst transfer (conventional strategy)?
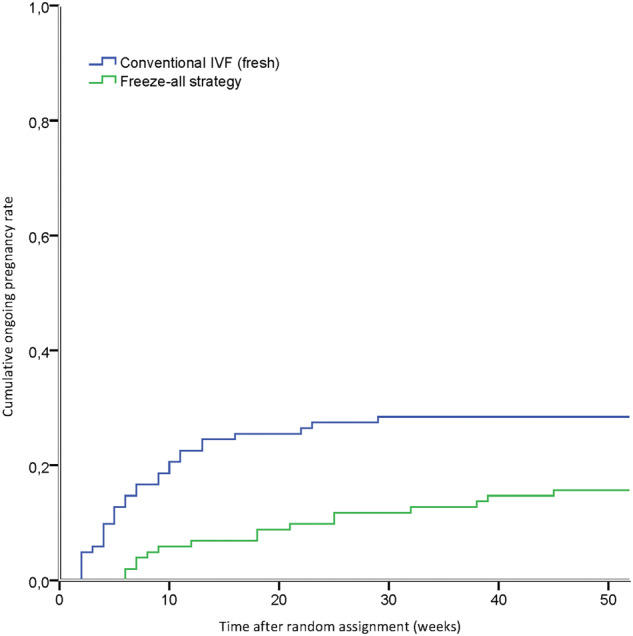
Summary answer: The freeze-all strategy was inferior to the conventional strategy in terms of cumulative ongoing pregnancy rate per woman.
What is known already: IVF without transfer of fresh embryos, thus with frozen-thawed embryo transfer only (freeze-all strategy), is increasingly being used in clinical practice because of a presumed benefit. It is still unknown whether this new IVF strategy increases IVF efficacy.
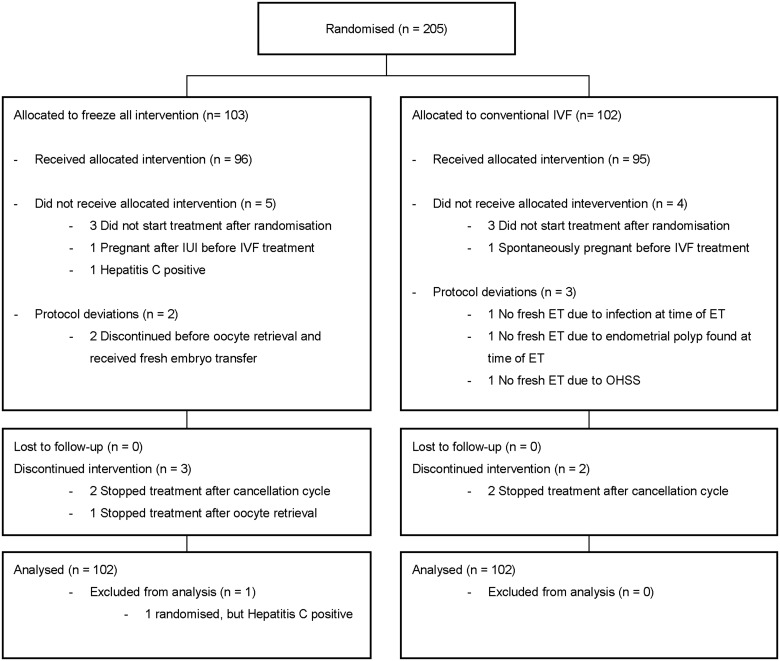
Study design, size, duration: A single-centre, open label, two arm, parallel group, randomised controlled superiority trial was conducted. The trial was conducted between January 2013 and July 2015 in the Netherlands. The intervention was one IVF cycle with frozen-thawed blastocyst transfer(s) versus one IVF cycle with fresh and frozen-thawed blastocyst transfer(s). The primary outcome was cumulative ongoing pregnancy resulting from one IVF cycle within 12 months after randomisation. Couples were allocated in a 1:1 ratio to the freeze-all strategy or the conventional strategy with an online randomisation programme just before the start of down-regulation.
Participants/materials, setting, methods: Participants were subfertile couples with any indication for IVF undergoing their first IVF cycle, with a female age between 18 and 43 years. Differences in cumulative ongoing pregnancy rates were expressed as relative risks (RR) with 95% CI. All outcomes were analysed following the intention-to-treat principle.
Main results and the role of chance: Two-hundred-and-five couples were randomly assigned to the freeze-all strategy (n = 102) or to the conventional strategy (n = 102). The cumulative ongoing pregnancy rate per woman was significantly lower in women allocated to the freeze-all strategy (19/102 (19%)) compared to women allocated to the conventional strategy (32/102 (31%); RR 0.59; 95% CI 0.36-0.98).
Limitations, reasons for caution: As this was a single-centre study, we were unable to study differences in study protocols and clinic performance. This, and the limited sample size, should make one cautious in using the results as the basis for definitive policy. All patients undergoing IVF, including those with a poor prognosis, were included; therefore, the outcome could differ in women with a good prognosis of IVF treatment success.
Wider implications of the findings: Our results indicate that there might be no benefit of a freeze-all strategy in terms of cumulative ongoing pregnancy rates. The efficacy of the freeze-all strategy in subgroups of patients, different stages of embryo development, and different freezing protocols needs to be further established and balanced against potential benefits and harms for mothers and children.
Study funding/competing interest(s): The Netherlands Organisation for Health Research and Development (ZonMW grant 171101007). S.M., F.M. and M.v.W. stated they are authors of the Cochrane review 'Fresh versus frozen embryo transfers in assisted reproduction'.
Trial registration number: Dutch Trial Register, NTR3187.
Trial registration date: 9 December 2011.
Date of first patient’s enrolment: 8 January 2013.
Keywords: ICSI; IVF; cryopreservation; embryo transfer; endometrium; freeze all; randomised controlled trial.
© The Author(s) 2021. Published by Oxford University Press on behalf of European Society of Human Reproduction and Embryology.
Figures
Comment in
-
Is the 'freeze-all' strategy really inferior to a 'fresh embryo transfer' strategy? Critical assessment of a randomized controlled trial.Hum Reprod. 2021 Jul 19;36(8):2418-2419. doi: 10.1093/humrep/deab116. Hum Reprod. 2021. PMID: 33993250 No abstract available.
-
Reply: Freeze-all vs conventional IVF: a valid and valuable RCT.Hum Reprod. 2021 Jul 19;36(8):2419-2420. doi: 10.1093/humrep/deab113. Hum Reprod. 2021. PMID: 33993251 No abstract available.
-
Is a randomized controlled design sufficient for a trial to be valuable?Hum Reprod. 2021 Jul 19;36(8):2416-2417. doi: 10.1093/humrep/deab114. Hum Reprod. 2021. PMID: 33993295 No abstract available.
-
Freeze-all or conventional IVF? Unanswered question from unlearned lessons.Hum Reprod. 2021 Jul 19;36(8):2417-2418. doi: 10.1093/humrep/deab115. Hum Reprod. 2021. PMID: 33993300 No abstract available.
References
-
- Aflatoonian A, Mansoori-Torshizi M, Farid Mojtahedi M, Aflatoonian B, Khalili MA, Amir-Arjmand MH, Soleimani M, Aflatoonian N, Oskouian H, Tabibnejad N. et al. Fresh versus frozen embryo transfer after gonadotropin-releasing hormone agonist trigger in gonadotropin-releasing hormone antagonist cycles among high responder women: a randomized, multi-center study. Int J Reprod Biomed 2018;16:9–18. - PMC - PubMed
-
- Amso NN, Ahuia KK, Morris N, Shaw RW.. Elective preembryo cryopreservation in ovarian hyperstimulation syndrome. J Assist Reprod Genet 1989;6:312–314. - PubMed
-
- Braakhekke M, , Kamphuis EI, , Dancet EA, , Mol F, , Van Der Veen F, , Mol BW. Ongoing pregnancy qualifies best as the primary outcome measure of choice in trials in reproductive medicine: an opinion paper. Fertil Steril 2014;101:1203–1204. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
