

Neuroanatomical Substrates and Symptoms Associated With Magnetic Resonance Imaging of Patients With Mild Traumatic Brain Injury
- PMID: 33734414
- PMCID: PMC7974642
- DOI: 10.1001/jamanetworkopen.2021.0994
Neuroanatomical Substrates and Symptoms Associated With Magnetic Resonance Imaging of Patients With Mild Traumatic Brain Injury
Abstract
Importance: Persistent symptoms after mild traumatic brain injury (mTBI) represent a major public health problem.
Objective: To identify neuroanatomical substrates of mTBI and the optimal timing for magnetic resonance imaging (MRI).
Design, setting, and participants: This prospective multicenter cohort study encompassed all eligible patients from the Collaborative European NeuroTrauma Effectiveness Research in Traumatic Brain Injury (CENTER-TBI) study (December 19, 2014, to December 17, 2017) and a local cohort (November 20, 2012, to December 19, 2013). Patients presented to the hospital within 24 hours of an mTBI (Glasgow Coma Score, 13-15), satisfied local criteria for computed tomographic scanning, and underwent MRI scanning less than 72 hours (MR1) and 2 to 3 weeks (MR2) after injury. In addition, 104 control participants were enrolled across all sites. Data were analyzed from January 1, 2019, to December 31, 2020.
Exposure: Mild TBI.
Main outcomes and measures: Volumes and diffusion parameters were extracted via automated bespoke pipelines. Symptoms were measured using the Rivermead Post Concussion Symptoms Questionnaire in the short term and the extended Glasgow Outcome Scale at 3 months.
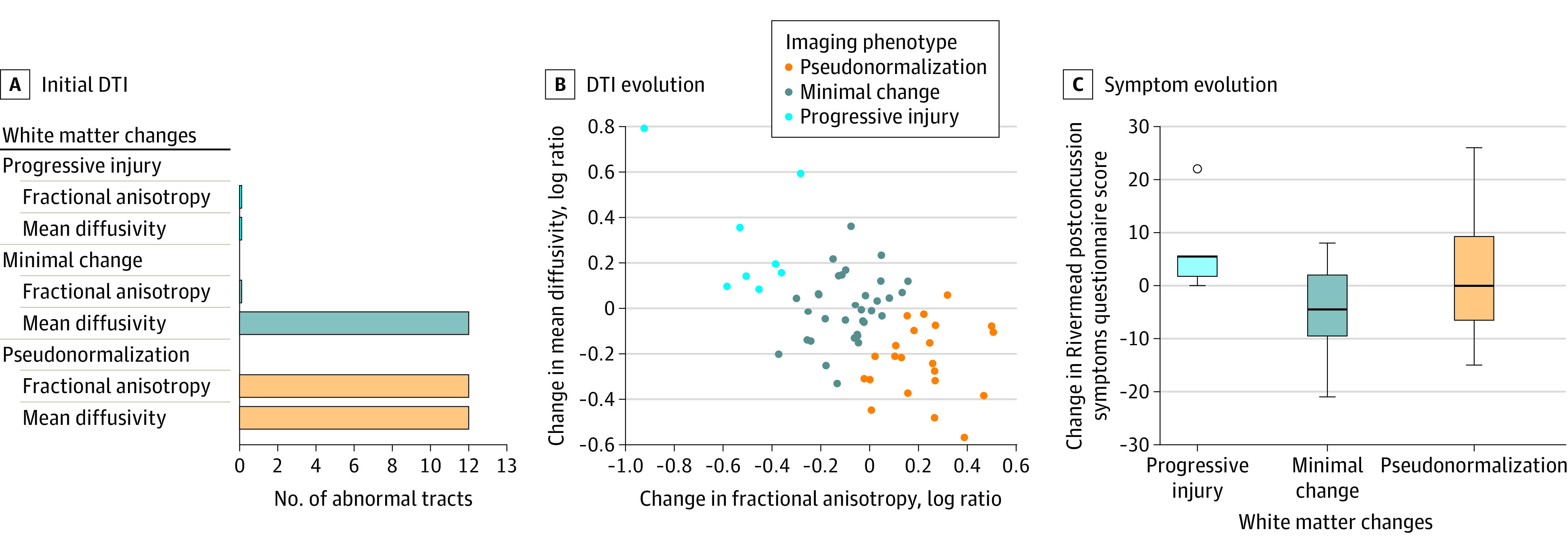
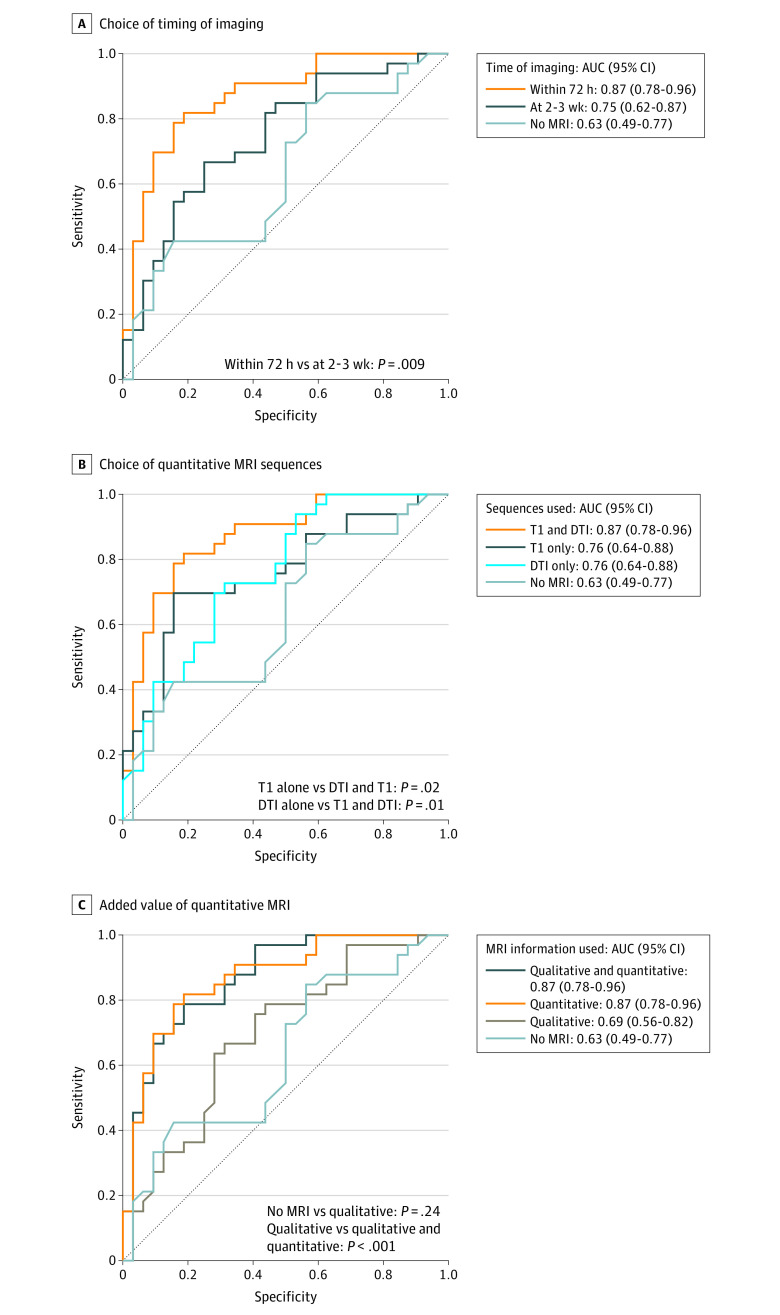
Results: Among the 81 patients included in the analysis (73 CENTER-TBI and 8 local), the median age was 45 (interquartile range [IQR], 24-59; range, 14-85) years, and 57 (70.4%) were male. Structural sequences were available for all scans; diffusion data, for 73 MR1 and 79 MR2 scans. After adjustment for multiple comparisons between scans, visible lesions did not differ significantly, but cerebral white matter volume decreased (MR2:MR1 ratio, 0.98; 95% CI, 0.96-0.99) and ventricular volume increased (MR2:MR1 ratio, 1.06; 95% CI, 1.02-1.10). White matter volume was within reference limits on MR1 scans (patient to control ratio, 0.99; 95% CI, 0.97-1.01) and reduced on MR2 scans (patient to control ratio, 0.97; 95% CI, 0.95-0.99). Diffusion parameters changed significantly between scans in 13 tracts, following 1 of 3 trajectories. Symptoms measured by Rivermead Post Concussion Symptoms Questionnaire scores worsened in the progressive injury phenotype (median, +5.00; IQR, +2.00 to +5.00]), improved in the minimal change phenotype (median, -4.50; IQR, -9.25 to +1.75), and were variable in the pseudonormalization phenotype (median, 0.00; IQR, -6.25 to +9.00) (P = .02). Recovery was favorable for 33 of 65 patients (51%) and was more closely associated with MR1 than MR2 (area under the curve, 0.87 [95% CI, 0.78-0.96] vs 0.75 [95% CI, 0.62-0.87]; P = .009).
Conclusions and relevance: These findings suggest that advanced MRI reveals potential neuroanatomical substrates of mTBI in white matter and is most strongly associated with odds of recovery if performed within 72 hours, although future validation is required.
Conflict of interest statement
Figures
Comment in
-
The Prognostic Role of Magnetic Resonance Imaging Biomarkers in Mild Traumatic Injury.JAMA Netw Open. 2021 Mar 1;4(3):e211824. doi: 10.1001/jamanetworkopen.2021.1824. JAMA Netw Open. 2021. PMID: 33734409 No abstract available.
Similar articles
-
Diffusion Tensor Imaging Reveals Elevated Diffusivity of White Matter Microstructure that Is Independently Associated with Long-Term Outcome after Mild Traumatic Brain Injury: A TRACK-TBI Study.J Neurotrauma. 2022 Oct;39(19-20):1318-1328. doi: 10.1089/neu.2021.0408. Epub 2022 Jul 18. J Neurotrauma. 2022. PMID: 35579949 Free PMC article.
-
Association of Sex and Age With Mild Traumatic Brain Injury-Related Symptoms: A TRACK-TBI Study.JAMA Netw Open. 2021 Apr 1;4(4):e213046. doi: 10.1001/jamanetworkopen.2021.3046. JAMA Netw Open. 2021. PMID: 33822070 Free PMC article.
-
MRI and Clinical Variables for Prediction of Outcomes After Pediatric Severe Traumatic Brain Injury.JAMA Netw Open. 2024 Aug 1;7(8):e2425765. doi: 10.1001/jamanetworkopen.2024.25765. JAMA Netw Open. 2024. PMID: 39102267 Free PMC article.
-
Magnetic Resonance Imaging Application in the Area of Mild and Acute Traumatic Brain Injury: Implications for Diagnostic Markers?In: Kobeissy FH, editor. Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects. Boca Raton (FL): CRC Press/Taylor & Francis; 2015. Chapter 24. In: Kobeissy FH, editor. Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects. Boca Raton (FL): CRC Press/Taylor & Francis; 2015. Chapter 24. PMID: 26269902 Free Books & Documents. Review.
-
Neuropathology of Mild Traumatic Brain Injury: Correlation to Neurocognitive and Neurobehavioral Findings.In: Kobeissy FH, editor. Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects. Boca Raton (FL): CRC Press/Taylor & Francis; 2015. Chapter 31. In: Kobeissy FH, editor. Brain Neurotrauma: Molecular, Neuropsychological, and Rehabilitation Aspects. Boca Raton (FL): CRC Press/Taylor & Francis; 2015. Chapter 31. PMID: 26269912 Free Books & Documents. Review.
Cited by
-
Anisotropy component of DTI reveals long-term neuroinflammation following repetitive mild traumatic brain injury in rats.Eur Radiol Exp. 2024 Jul 24;8(1):82. doi: 10.1186/s41747-024-00490-w. Eur Radiol Exp. 2024. PMID: 39046630 Free PMC article.
-
Trajectories of brain volumes in young children are associated with maternal education.Hum Brain Mapp. 2023 Jun 1;44(8):3168-3179. doi: 10.1002/hbm.26271. Epub 2023 Mar 10. Hum Brain Mapp. 2023. PMID: 36896867 Free PMC article.
-
Serum lipidome associates with neuroimaging features in patients with traumatic brain injury.iScience. 2024 Aug 3;27(9):110654. doi: 10.1016/j.isci.2024.110654. eCollection 2024 Sep 20. iScience. 2024. PMID: 39252979 Free PMC article.
-
Integrative Neuroinformatics for Precision Prognostication and Personalized Therapeutics in Moderate and Severe Traumatic Brain Injury.Front Neurol. 2021 Sep 7;12:729184. doi: 10.3389/fneur.2021.729184. eCollection 2021. Front Neurol. 2021. PMID: 34557154 Free PMC article. Review.
-
Post-Concussive Vestibular Dysfunction Is Related to Injury to the Inferior Vestibular Nerve.J Neurotrauma. 2022 Jun;39(11-12):829-840. doi: 10.1089/neu.2021.0447. Epub 2022 Mar 7. J Neurotrauma. 2022. PMID: 35171721 Free PMC article.
References
-
- Steyerberg EW, Wiegers E, Sewalt C, et al. ; CENTER-TBI Participants and Investigators . Case-mix, care pathways, and outcomes in patients with traumatic brain injury in CENTER-TBI: a European prospective, multicentre, longitudinal, cohort study. Lancet Neurol. 2019;18(10):923-934. doi:10.1016/S1474-4422(19)30232-7 - DOI - PubMed
-
- Nelson LD, Temkin NR, Dikmen S, et al. ; TRACK-TBI Investigators . Recovery after mild traumatic brain injury in patients presenting to US level I trauma centers: a Transforming Research and Clinical Knowledge in Traumatic Brain Injury (TRACK-TBI) study. JAMA Neurol. 2019;76(9):1049-1059. doi:10.1001/jamaneurol.2019.1313 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
