

Predictive factors for long-term survival after surgery for pancreatic ductal adenocarcinoma: Making a case for standardized reporting of the resection margin using certified cancer center data
- PMID: 33735191
- PMCID: PMC7971889
- DOI: 10.1371/journal.pone.0248633
Predictive factors for long-term survival after surgery for pancreatic ductal adenocarcinoma: Making a case for standardized reporting of the resection margin using certified cancer center data
Abstract
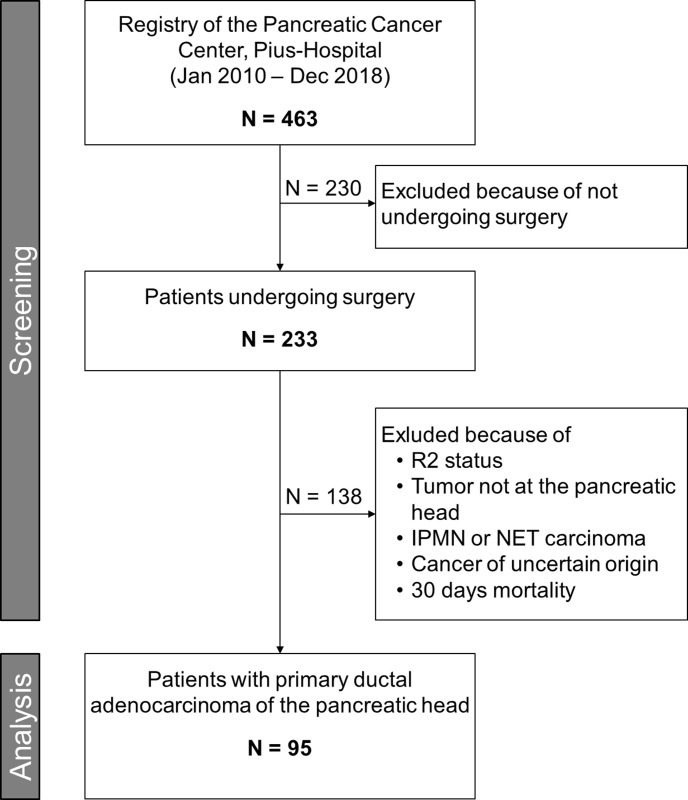
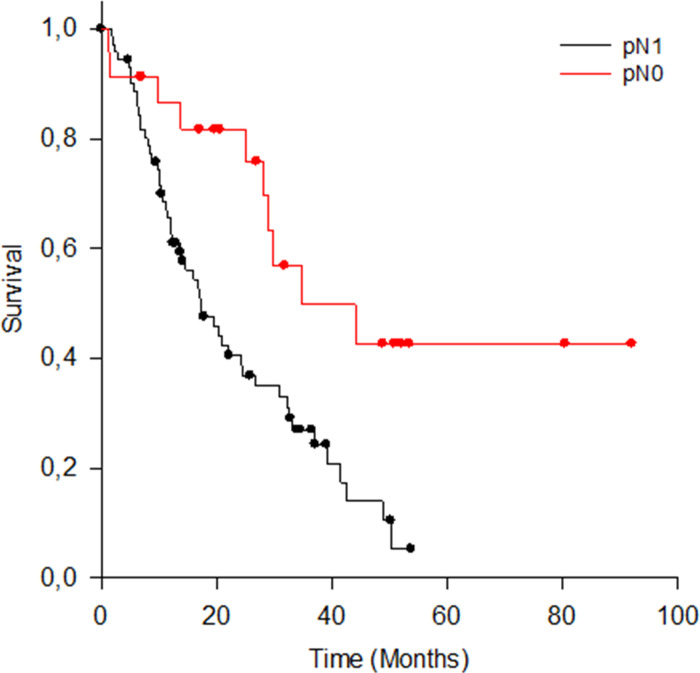
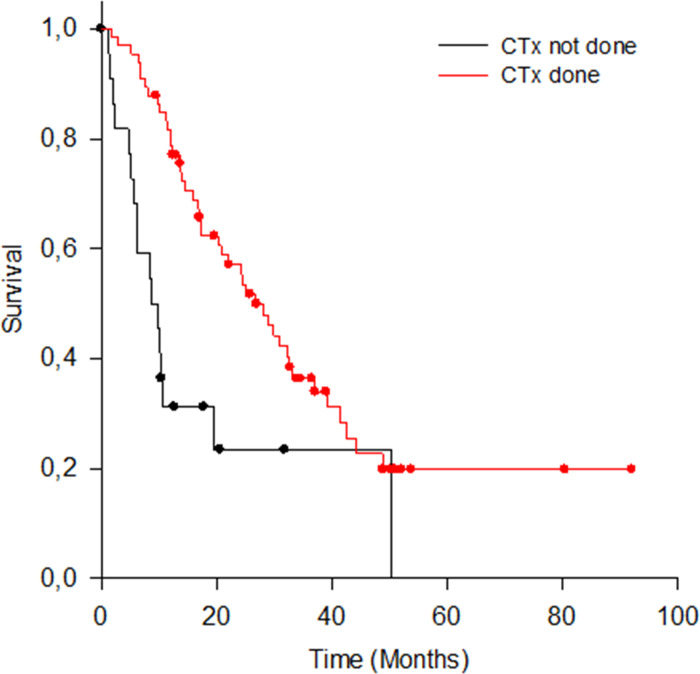
Factors for overall survival after pancreatic ductal adenocarcinoma (PDAC) seem to be nodal status, chemotherapy administration, UICC staging, and resection margin. However, there is no consensus on the definition for tumor free resection margin. Therefore, univariate OS as well as multivariate long-term survival using cancer center data was analyzed with regards to two different resection margin definitions. Ninety-five patients met inclusion criteria (pancreatic head PDAC, R0/R1, no 30 days mortality). OS was analyzed in univariate analysis with respect to R-status, CRM (circumferential resection margin; positive: ≤1mm; negative: >1mm), nodal status, and chemotherapy administration. Long-term survival >36 months was modelled using multivariate logistic regression instead of Cox regression because the distribution function of the dependent data violated the requirements for the application of this test. Significant differences in OS were found regarding the R status (Median OS and 95%CI for R0: 29.8 months, 22.3-37.4; R1: 15.9 months, 9.2-22.7; p = 0.005), nodal status (pN0 = 34.7, 10.4-59.0; pN1 = 17.1, 11.5-22.8; p = 0.003), and chemotherapy (with CTx: 26.7, 20.4-33.0; without CTx: 9.7, 5.2-14.1; p < .001). OS according to CRM status differed on a clinically relevant level by about 12 months (CRM positive: 17.2 months, 11.5-23.0; CRM negative: 29.8 months, 18.6-41.1; p = 0.126). A multivariate model containing chemotherapy, nodal status, and CRM explained long-term survival (p = 0.008; correct prediction >70%). Chemotherapy, nodal status and resection margin according to UICC R status are univariate factors for OS after PDAC. In contrast, long-term survival seems to depend on wider resection margins than those used in UICC R classification. Therefore, standardized histopathological reporting (including resection margin size) should be agreed upon.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




References
-
- Kayahara M, Nagakawa T, Ueno K, Ohta T, Takeda T, Miyazaki I. An evaluation of radical resection for pancreatic cancer based on the mode of recurrence as determined by autopsy and diagnostic imaging. Cancer. 1993;72(7):2118–23. 10.1002/1097-0142(19931001)72:7<2118::aid-cncr2820720710>3.0.co;2-4 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
