

Clinical decision-making in older adults following emergency admission to hospital. Derivation and validation of a risk stratification score: OPERA
- PMID: 33735316
- PMCID: PMC7971558
- DOI: 10.1371/journal.pone.0248477
Clinical decision-making in older adults following emergency admission to hospital. Derivation and validation of a risk stratification score: OPERA
Abstract
Objectives of the study: Demographic changes alongside medical advances have resulted in older adults accounting for an increasing proportion of emergency hospital admissions. Current measures of illness severity, limited to physiological parameters, have shortcomings in this cohort, partly due to patient complexity. This study aimed to derive and validate a risk score for acutely unwell older adults which may enhance risk stratification and support clinical decision-making.
Methods: Data was collected from emergency admissions in patients ≥65 years from two UK general hospitals (April 2017- April 2018). Variables underwent regression analysis for in-hospital mortality and independent predictors were used to create a risk score. Performance was assessed on external validation. Secondary outcomes included seven-day mortality and extended hospital stay.
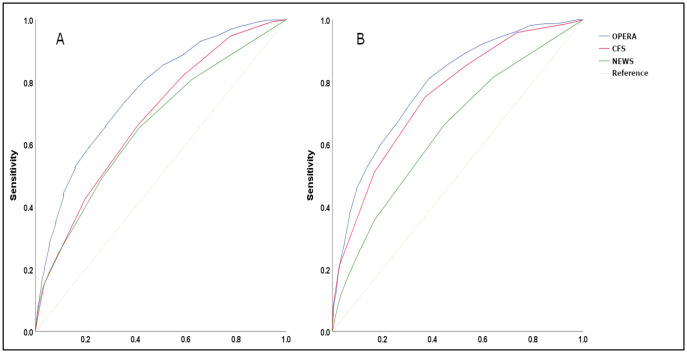
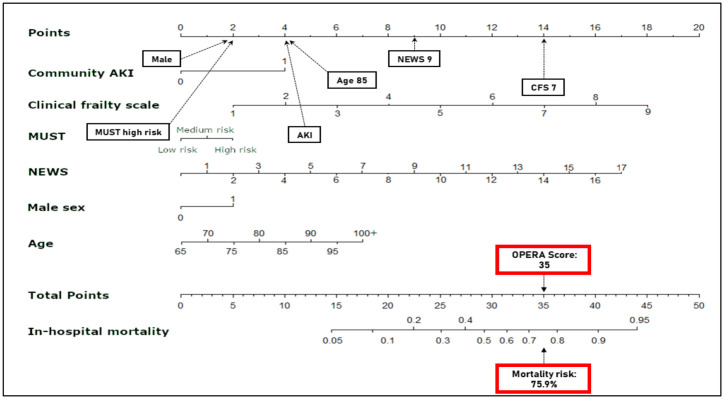
Results: Derivation (n = 8,974) and validation (n = 8,391) cohorts were analysed. The model included the National Early Warning Score 2 (NEWS2), clinical frailty scale (CFS), acute kidney injury, age, sex, and Malnutrition Universal Screening Tool. For mortality, area under the curve for the model was 0.79 (95% CI 0.78-0.80), superior to NEWS2 0.65 (0.62-0.67) and CFS 0.76 (0.74-0.77) (P<0.0001). Risk groups predicted prolonged hospital stay: the highest risk group had an odds ratio of 9.7 (5.8-16.1) to stay >30 days.
Conclusions: Our simple validated model (Older Persons' Emergency Risk Assessment [OPERA] score) predicts in-hospital mortality and prolonged length of stay and could be easily integrated into electronic hospital systems, enabling automatic digital generation of risk stratification within hours of admission. Future studies may validate the OPERA score in external populations and consider an impact analysis.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
National Early Warning Score 2 (NEWS2) on admission predicts severe disease and in-hospital mortality from Covid-19 - a prospective cohort study.Scand J Trauma Resusc Emerg Med. 2020 Jul 13;28(1):66. doi: 10.1186/s13049-020-00764-3. Scand J Trauma Resusc Emerg Med. 2020. PMID: 32660623 Free PMC article.
-
Development and validation of a novel computer-aided score to predict the risk of in-hospital mortality for acutely ill medical admissions in two acute hospitals using their first electronically recorded blood test results and vital signs: a cross-sectional study.BMJ Open. 2018 Dec 6;8(12):e022939. doi: 10.1136/bmjopen-2018-022939. BMJ Open. 2018. PMID: 30530474 Free PMC article.
-
National Early Warning Score 2 (NEWS2) and 3-level triage scale as risk predictors in frail older adults in the emergency department.BMC Emerg Med. 2020 Oct 28;20(1):83. doi: 10.1186/s12873-020-00379-y. BMC Emerg Med. 2020. PMID: 33115446 Free PMC article.
-
Modifications to the National Early Warning Score 2: a Scoping Review.BMC Med. 2025 Mar 11;23(1):154. doi: 10.1186/s12916-025-03943-0. BMC Med. 2025. PMID: 40069742 Free PMC article.
-
Effectiveness of Early Warning Scores for Early Severity Assessment in Outpatient Emergency Care: A Systematic Review.Front Public Health. 2022 Jul 14;10:894906. doi: 10.3389/fpubh.2022.894906. eCollection 2022. Front Public Health. 2022. PMID: 35910902 Free PMC article.
Cited by
-
What can we learn from 68 000 clinical frailty scale scores? Evaluating the utility of frailty assessment in emergency departments.Age Ageing. 2025 Mar 28;54(4):afaf093. doi: 10.1093/ageing/afaf093. Age Ageing. 2025. PMID: 40253684 Free PMC article.
-
Acute Kidney Injury Following Posaconazole for Mucormycosis: SARS-CoV-2 as a Back-Seat Driver.Cureus. 2022 Jul 19;14(7):e27018. doi: 10.7759/cureus.27018. eCollection 2022 Jul. Cureus. 2022. PMID: 35989786 Free PMC article.
References
-
- Wittenberg R, Sharpin L, McCormick B, Hurst J. Understanding emergency hospital admission of older people. 2014. https://www.chseo.org.uk/downloads/report6-emergencyadmissions.pdf
-
- Baillie L, Gallini A, Corser R, Elworthy G, Scotcher A, Barrand A. Care transitions for frail, older people from acute hospital wards within an integrated healthcare system in England: a qualitative case study. International Journal of Integrated Care. 2014;14. 10.5334/ijic.1175 - DOI - PMC - PubMed
-
- Royal College of Physicians. National early warning score (NEWS) 2. Standardising the assessment of acute-illness severity in the NHS. 2017. https://www.rcplondon.ac.uk/projects/outputs/national-early-warning-scor...
-
- de Groot B, Stolwijk F, Warmerdam M, Lucke JA, Singh GK, Abbas M, et al.. The most commonly used disease severity scores are inappropriate for risk stratification of older emergency department sepsis patients: an observational multi-centre study. Scandinavian journal of trauma, resuscitation and emergency medicine. 2017;25(1):91. 10.1186/s13049-017-0436-3 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
