

First-line antiepileptic drug treatment in glioma patients with epilepsy: Levetiracetam vs valproic acid
- PMID: 33735464
- PMCID: PMC8251728
- DOI: 10.1111/epi.16880
First-line antiepileptic drug treatment in glioma patients with epilepsy: Levetiracetam vs valproic acid
Abstract
Objective: This study aimed at estimating the cumulative incidence of antiepileptic drug (AED) treatment failure of first-line monotherapy levetiracetam vs valproic acid in glioma patients with epilepsy.
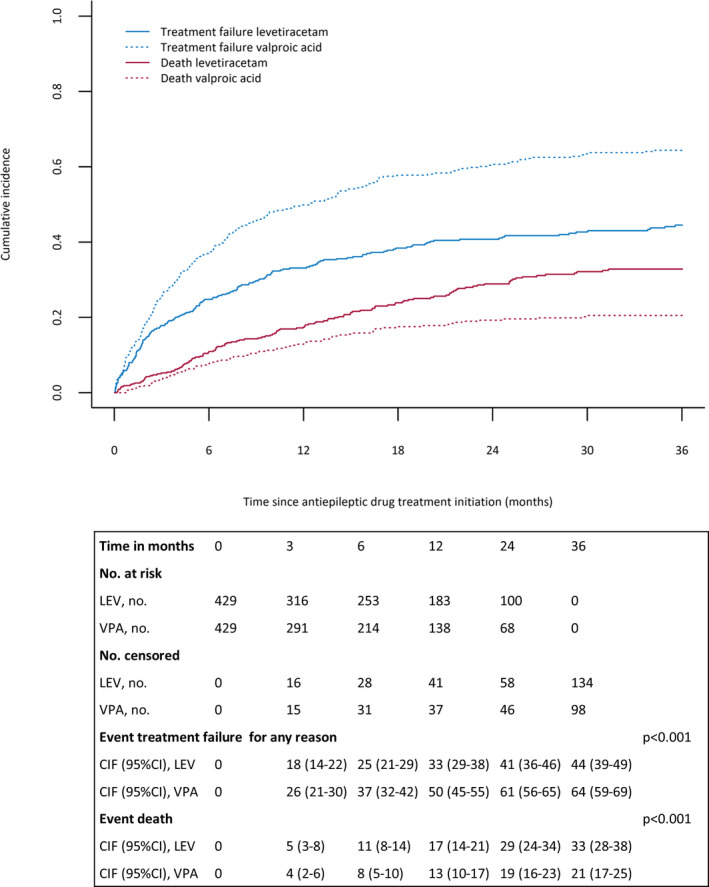
Methods: In this retrospective observational study, a competing risks model was used to estimate the cumulative incidence of treatment failure, from AED treatment initiation, for the two AEDs with death as a competing event. Patients were matched on baseline covariates potentially related to treatment assignment and outcomes of interest according to the nearest neighbor propensity score matching technique. Maximum duration of follow-up was 36 months.
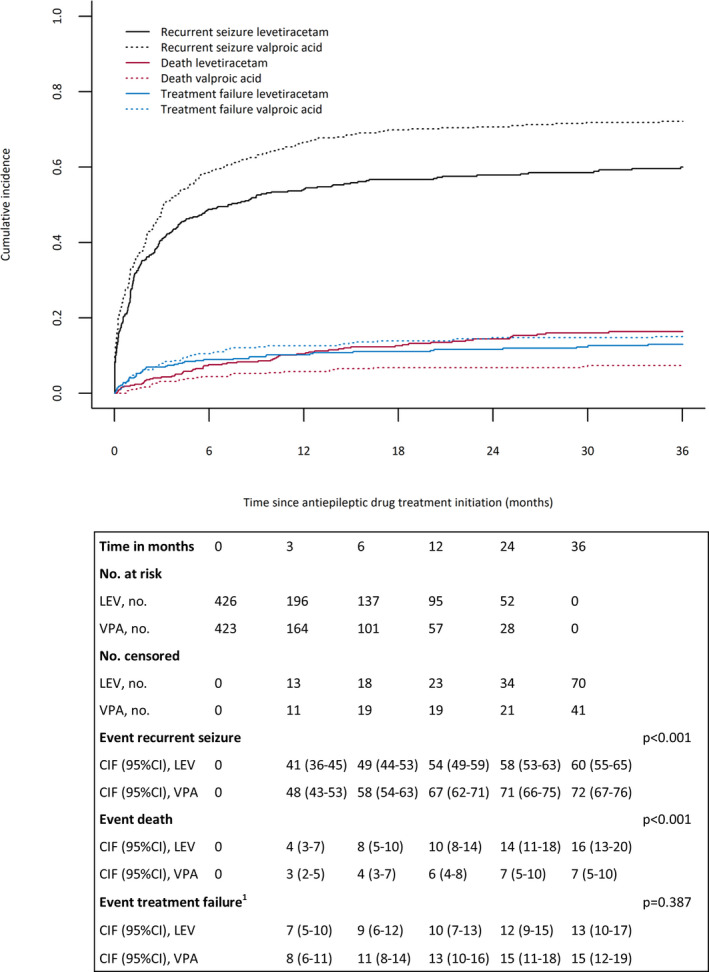
Results: In total, 776 patients using levetiracetam and 659 using valproic acid were identified. Matching resulted in two equal groups of 429 patients, with similar covariate distribution. The cumulative incidence of treatment failure for any reason was significantly lower for levetiracetam compared to valproic acid (12 months: 33% [95% confidence interval (CI) 29%-38%] vs 50% [95% CI 45%-55%]; P < .001). When looking at specific reasons of treatment failure, treatment failure due to uncontrolled seizures was significantly lower for levetiracetam compared to valproic acid (12 months: 16% [95% CI 12%-19%] vs 28% [95% CI 23%-32%]; P < 0.001), but no differences were found for treatment failure due to adverse effects (12 months: 14% [95% CI 11%-18%] vs 15% [95% CI 11%-18%]; P = .636).
Significance: Our results suggest that levetiracetam may have favorable efficacy compared to valproic acid, whereas level of toxicity seems similar. Therefore, levetiracetam seems to be the preferred choice for first-line AED treatment in patients with glioma.
Keywords: antiepileptic drug; glioma; levetiracetam; seizures; valproic acid.
© 2021 The Authors. Epilepsia published by Wiley Periodicals LLC on behalf of International League Against Epilepsy.
Conflict of interest statement
None of the authors declare a conflict of interest. We confirm that we have read the Journal's guidelines for ethical publication and affirm that this manuscript is consistent with these guidelines.
Figures
Similar articles
-
Antiseizure medication choice in diffuse glioma: A single-center population-based experience.Epilepsia Open. 2025 Jun;10(3):705-716. doi: 10.1002/epi4.70007. Epub 2025 Apr 30. Epilepsia Open. 2025. PMID: 40308033 Free PMC article.
-
Efficacy of anti-epileptic drugs in patients with gliomas and seizures.J Neurol. 2009 Sep;256(9):1519-26. doi: 10.1007/s00415-009-5156-9. Epub 2009 May 12. J Neurol. 2009. PMID: 19434440
-
Levetiracetam compared with valproic acid for the prevention of postoperative seizures after supratentorial tumor surgery: a retrospective chart review.CNS Drugs. 2013 Sep;27(9):753-9. doi: 10.1007/s40263-013-0094-6. CNS Drugs. 2013. PMID: 23921717
-
Management of epilepsy in brain tumor patients.Curr Opin Oncol. 2022 Nov 1;34(6):685-690. doi: 10.1097/CCO.0000000000000876. Epub 2022 Jul 16. Curr Opin Oncol. 2022. PMID: 35838207 Free PMC article. Review.
-
Antiepileptic drugs as prophylaxis for postcraniotomy seizures.Cochrane Database Syst Rev. 2020 Apr 28;4(4):CD007286. doi: 10.1002/14651858.CD007286.pub5. Cochrane Database Syst Rev. 2020. PMID: 32343399 Free PMC article.
Cited by
-
Letter regarding "SNO and EANO practice guideline update: Anticonvulsant prophylaxis in patients with newly diagnosed brain tumors".Neuro Oncol. 2022 Mar 12;24(3):499-500. doi: 10.1093/neuonc/noab283. Neuro Oncol. 2022. PMID: 35079810 Free PMC article. No abstract available.
-
First-line levetiracetam versus enzyme-inducing antiseizure medication in glioma patients with epilepsy.Epilepsia. 2023 Jan;64(1):162-169. doi: 10.1111/epi.17464. Epub 2022 Nov 24. Epilepsia. 2023. PMID: 36380710 Free PMC article.
-
Impact of timing of antiseizure medication withdrawal on seizure recurrence in glioma patients: a retrospective observational study.J Neurooncol. 2023 Sep;164(3):545-555. doi: 10.1007/s11060-023-04450-z. Epub 2023 Sep 27. J Neurooncol. 2023. PMID: 37755633 Free PMC article.
-
The evolution of antiseizure medication therapy selection in adults: Is artificial intelligence -assisted antiseizure medication selection ready for prime time?J Cent Nerv Syst Dis. 2023 Oct 18;15:11795735231209209. doi: 10.1177/11795735231209209. eCollection 2023. J Cent Nerv Syst Dis. 2023. PMID: 37868934 Free PMC article. Review.
-
Effects of Levetiracetam and Lacosamide on survival and seizure control in IDH-wild type glioblastoma during temozolomide plus radiation adjuvant therapy.Brain Spine. 2023 Dec 14;4:102732. doi: 10.1016/j.bas.2023.102732. eCollection 2024. Brain Spine. 2023. PMID: 38510602 Free PMC article.
References
-
- Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella‐Branger D, Cavenee WK, et al. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. 2016;131:803–20. - PubMed
-
- Weller M, van den Bent M, Hopkins K, Tonn JC, Stupp R, Falini A, et al. EANO guideline for the diagnosis and treatment of anaplastic gliomas and glioblastoma. Lancet Oncol. 2014;15:e395–403. - PubMed
-
- Samudra N, Zacharias T, Plitt A, Lega B, Pan E. Seizures in glioma patients: An overview of incidence, etiology, and therapies. J Neurol Sci. 2019;404:80–5. - PubMed
-
- Phan K, Ng W, Lu VM, McDonald KL, Fairhall J, Reddy R, et al. Association between IDH1 and IDH2 mutations and preoperative seizures in patients with low‐grade versus high‐grade glioma: a systematic review and meta‐analysis. World Neurosurg. 2018;111:e539–e545. - PubMed
-
- Maschio M, Aguglia U, Avanzini G, Banfi P, Buttinelli C, Capovilla G, et al. Management of epilepsy in brain tumors. Neurol Sci. 2019;40:2217–34. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
