

A rapid genotyping panel for detection of primary central nervous system lymphoma
- PMID: 33735913
- PMCID: PMC8343545
- DOI: 10.1182/blood.2020010137
A rapid genotyping panel for detection of primary central nervous system lymphoma
Abstract
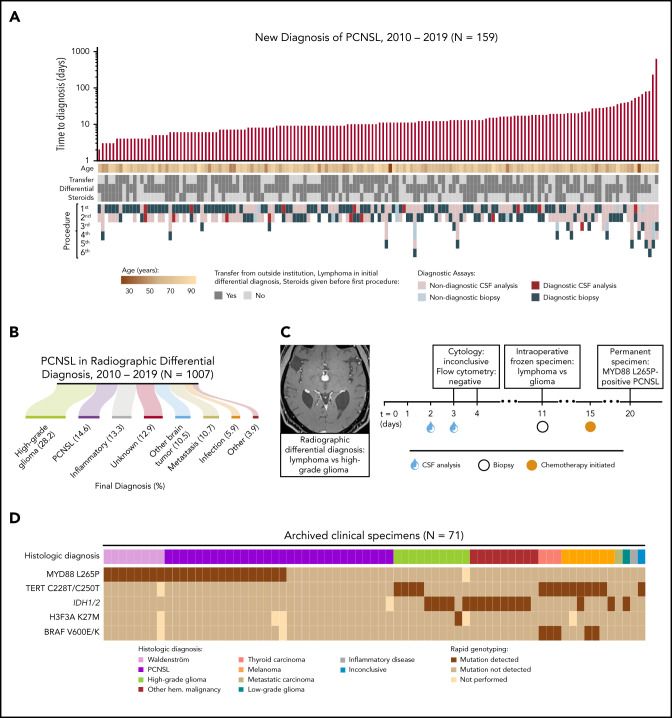
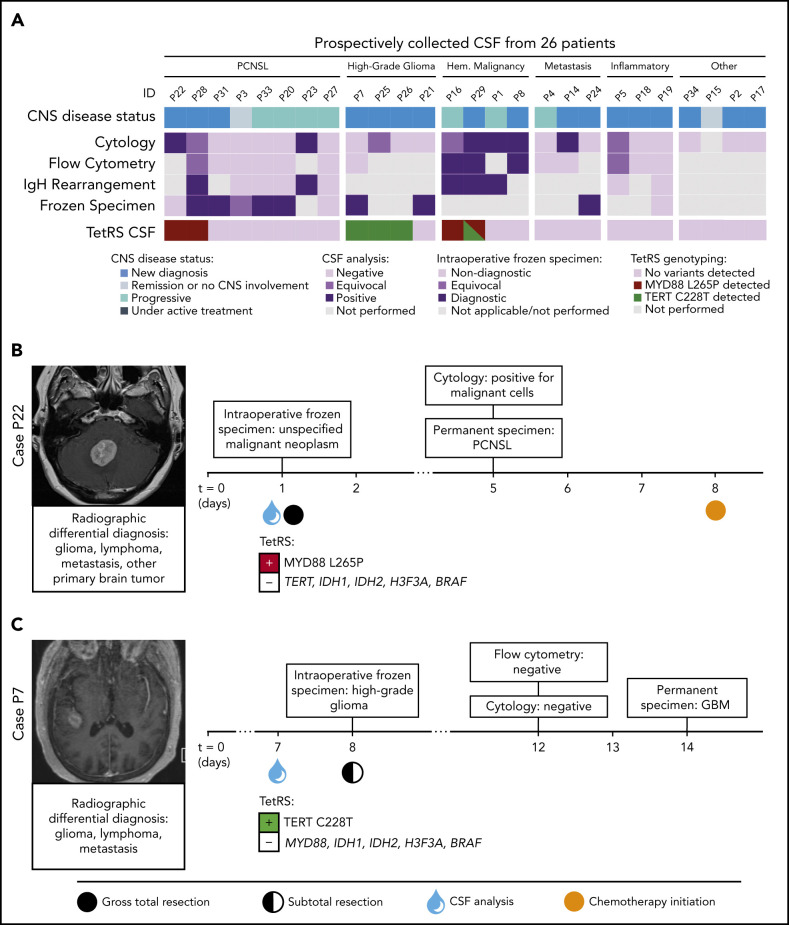
Diagnosing primary central nervous system lymphoma (PCNSL) frequently requires neurosurgical biopsy due to nonspecific radiologic features and the low yield of cerebrospinal fluid (CSF) studies. We characterized the clinical evaluation of suspected PCNSL (N = 1007 patients) and designed a rapid multiplexed genotyping assay for MYD88, TERT promoter, IDH1/2, H3F3A, and BRAF mutations to facilitate the diagnosis of PCNSL from CSF and detect other neoplasms in the differential diagnosis. Among 159 patients with confirmed PCNSL, the median time to secure a diagnosis of PCNSL was 10 days, with a range of 0 to 617 days. Permanent histopathology confirmed PCNSL in 142 of 152 biopsies (93.4%), whereas CSF analyses were diagnostic in only 15/113 samplings (13.3%). Among 86 archived clinical specimens, our targeted genotyping assay accurately detected hematologic malignancies with 57.6% sensitivity and 100% specificity (95% confidence interval [CI]: 44.1% to 70.4% and 87.2% to 100%, respectively). MYD88 and TERT promoter mutations were prospectively identified in DNA extracts of CSF obtained from patients with PCNSL and glioblastoma, respectively, within 80 minutes. Across 132 specimens, hallmark mutations indicating the presence of malignancy were detected with 65.8% sensitivity and 100% specificity (95% CI: 56.2%-74.5% and 83.9%-100%, respectively). This targeted genotyping approach offers a rapid, scalable adjunct to reduce diagnostic and treatment delays in PCNSL.
© 2021 by The American Society of Hematology.
Figures

References
-
- Cerqua R, Balestrini S, Perozzi C, et al. Diagnostic delay and prognosis in primary central nervous system lymphoma compared with glioblastoma multiforme. Neurol Sci 2016;37(1):23-29. - PubMed
-
- Han CH, Batchelor TT. Diagnosis and management of primary central nervous system lymphoma. Cancer 2017;123(22):4314-4324. - PubMed
-
- Canovi S, Campioli D. Accuracy of flow cytometry and cytomorphology for the diagnosis of meningeal involvement in lymphoid neoplasms: A systematic review. Diagn Cytopathol 2016;44(10):841-856. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
