

Frailty status as a potential factor in increased postoperative opioid use in older adults
- PMID: 33736611
- PMCID: PMC7977609
- DOI: 10.1186/s12877-021-02101-4
Frailty status as a potential factor in increased postoperative opioid use in older adults
Abstract
Background: Prescription opioids are commonly used for postoperative pain relief in older adults, but have the potential for misuse. Both opioid side effects and uncontrolled pain have detrimental impacts. Frailty syndrome (reduced reserve in response to stressors), pain, and chronic opioid consumption are all complex phenomena that impair function, nutrition, psychologic well-being, and increase mortality, but links among these conditions in the acute postoperative setting have not been described. This study seeks to understand the relationship between frailty and patterns of postoperative opioid consumption in older adults.
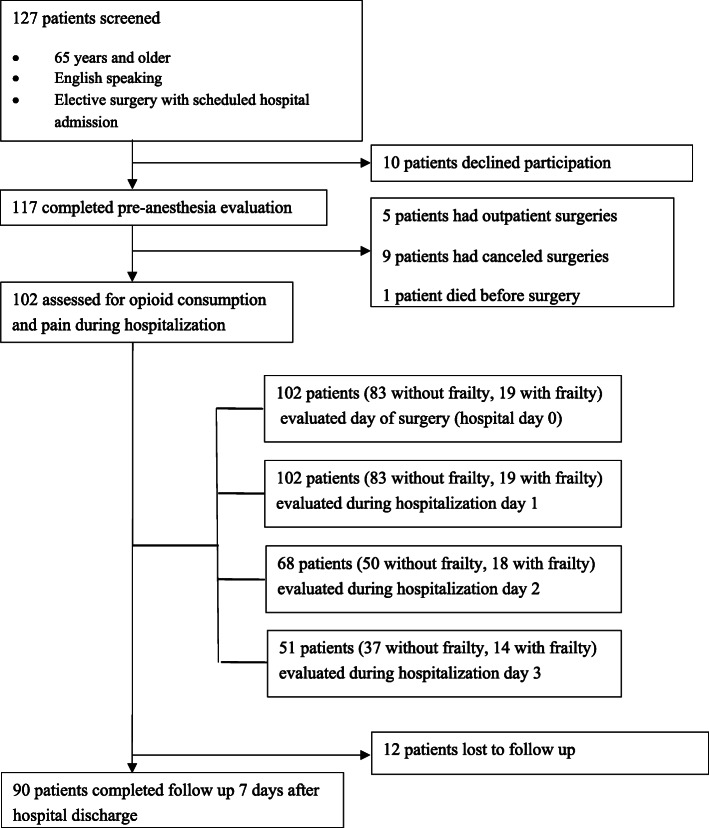
Methods: Patients ≥ 65 years undergoing elective surgery with a planned hospital stay of at least one postoperative day were recruited for this cohort study at pre-anesthesia clinic visits. Preoperatively, frailty was assessed by Edmonton Frailty and Clinical Frailty Scales, pain was assessed by Visual Analog and Pain Catastrophizing Scales, and opioid consumption was recorded. On the day of surgery and subsequent hospitalization days, average pain ratings and total opioid consumption were recorded daily. Seven days after hospital discharge, patients were interviewed using uniform questionnaires to measure opioid prescription use and pain rating.
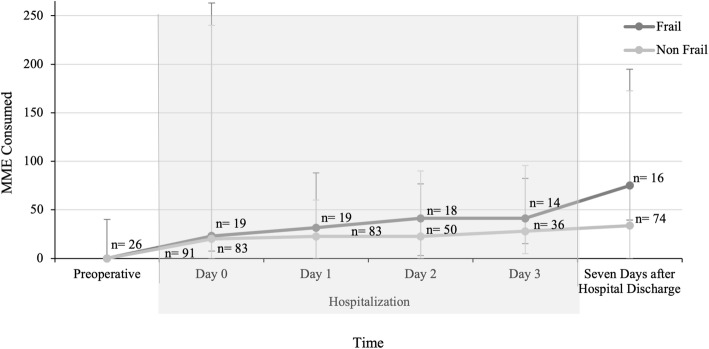
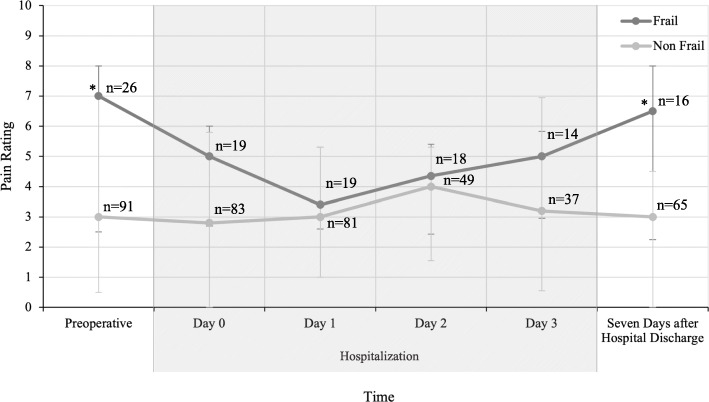
Results: One hundred seventeen patients (age 73.0 (IQR 67.0, 77.0), 64 % male), were evaluated preoperatively and 90 completed one-week post discharge follow-up. Preoperatively, patients with frailty were more likely than patients without frailty to use opioids (46.2 % vs. 20.9 %, p = 0.01). Doses of opioids prescribed at hospital discharge and the prescribed morphine milligram equivalents (MME) at discharge did not differ between groups. Seven days after discharge, the cumulative MME used were similar between cohorts. However, patients with frailty used a larger fraction of opioids prescribed to them (96.7 % (31.3, 100.0) vs. 25.0 % (0.0, 83.3), p = 0.007) and were more likely (OR 3.7, 95 % CI 1.13-12.13) to use 50 % and greater of opioids prescribed to them. Patients with frailty had higher pain scores before surgery and seven days after discharge compared to patients without frailty.
Conclusions: Patterns of postoperative opioid use after discharge were different between patients with and without frailty. Patients with frailty tended to use almost all the opioids prescribed while patients without frailty tended to use almost none of the opioids prescribed.
Conflict of interest statement
Elizabeth Auckley and Lily Jeong received funding from The Medical Student Training in Aging Research Program, the National Institute on Aging (T35AG026736), and the Lillian R. Gleitsman Foundation. This funding had no role in the study and these authors declare no conflict of interest. Nathalie Bentov, Shira Zelber-Sagi, May Reed, and Itay Bentov declare that they have no conflict of interest.
Figures


References
-
- Manchikanti L, Helm S, 2nd, Fellows B, Janata JW, Pampati V, Grider JS, et al. Opioid epidemic in the United States. Pain Physician. 2012;15(3 Suppl):ES9–38. - PubMed
-
- Murthy VH. Ending the opioid epidemic — a call to action. N Engl J Med. 2016;375(25):2413–5. - PubMed
-
- Department of Health & Human Services. (2016). Opioids in Medicare Part D: Concerns about extreme use and questionable prescribing. Office of the Inspector General. Retrieved from .
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
