

The trends and associated adverse maternal and perinatal outcomes of labour neuraxial analgesia among vaginal deliveries in China between 2012 and 2019: a real-world observational evidence
- PMID: 33736635
- PMCID: PMC7977606
- DOI: 10.1186/s12916-021-01941-6
The trends and associated adverse maternal and perinatal outcomes of labour neuraxial analgesia among vaginal deliveries in China between 2012 and 2019: a real-world observational evidence
Abstract
Background: There is a lack of national report of the labour neuraxial analgesia (NA) rates in China in recent years, especially after the national promotion policy. The adverse maternal and perinatal outcomes associated with NA in China are also unknown. The aim of this study is to estimate the trends of NA rates from 2012 to 2019, to evaluate the effect of national policy on promoting NA and to identify the association between NA and adverse outcomes in China.
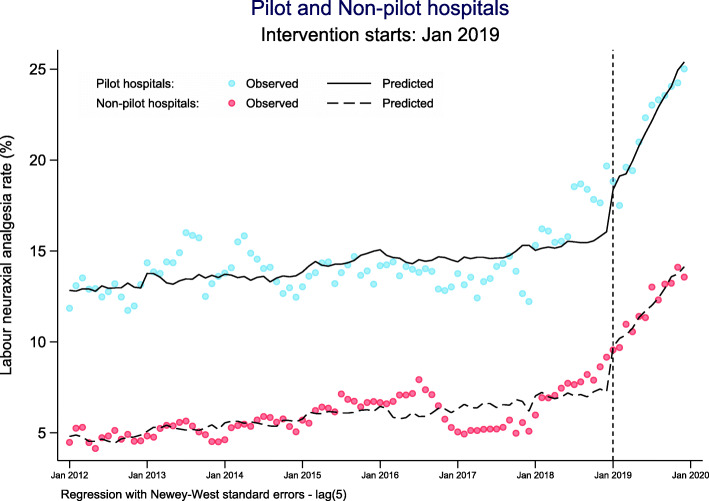
Methods: We used the individual data from China's National Maternal Near Miss Surveillance System (NMNMSS) between 2012 and 2019, covering 438 hospitals from 326 urban districts or rural counties in 30 provinces across China. The analysis was restricted to singleton pregnant women who underwent vaginal delivery at or after 28 completed weeks of gestation. We estimate the trends of NA rates between 2012 and 2019, both at the national and provincial levels using Bayesian multilevel model. We also estimated the effect of the national pilot policy launched in 2018 using interrupted time-series analysis and identified the association between NA and adverse outcomes using modified Poisson regression combined with propensity score analysis.
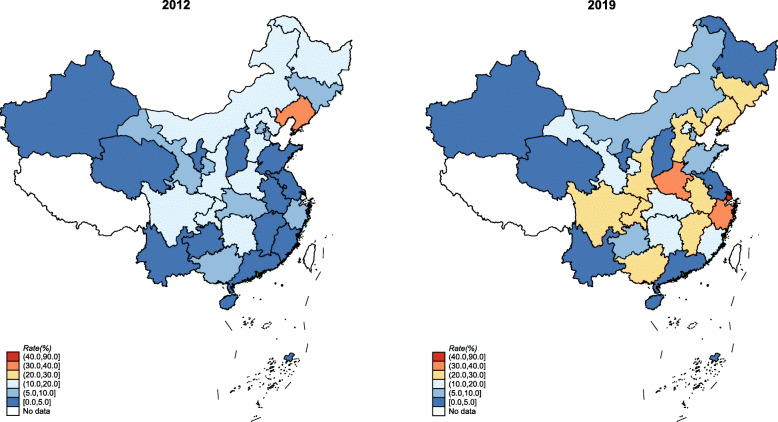
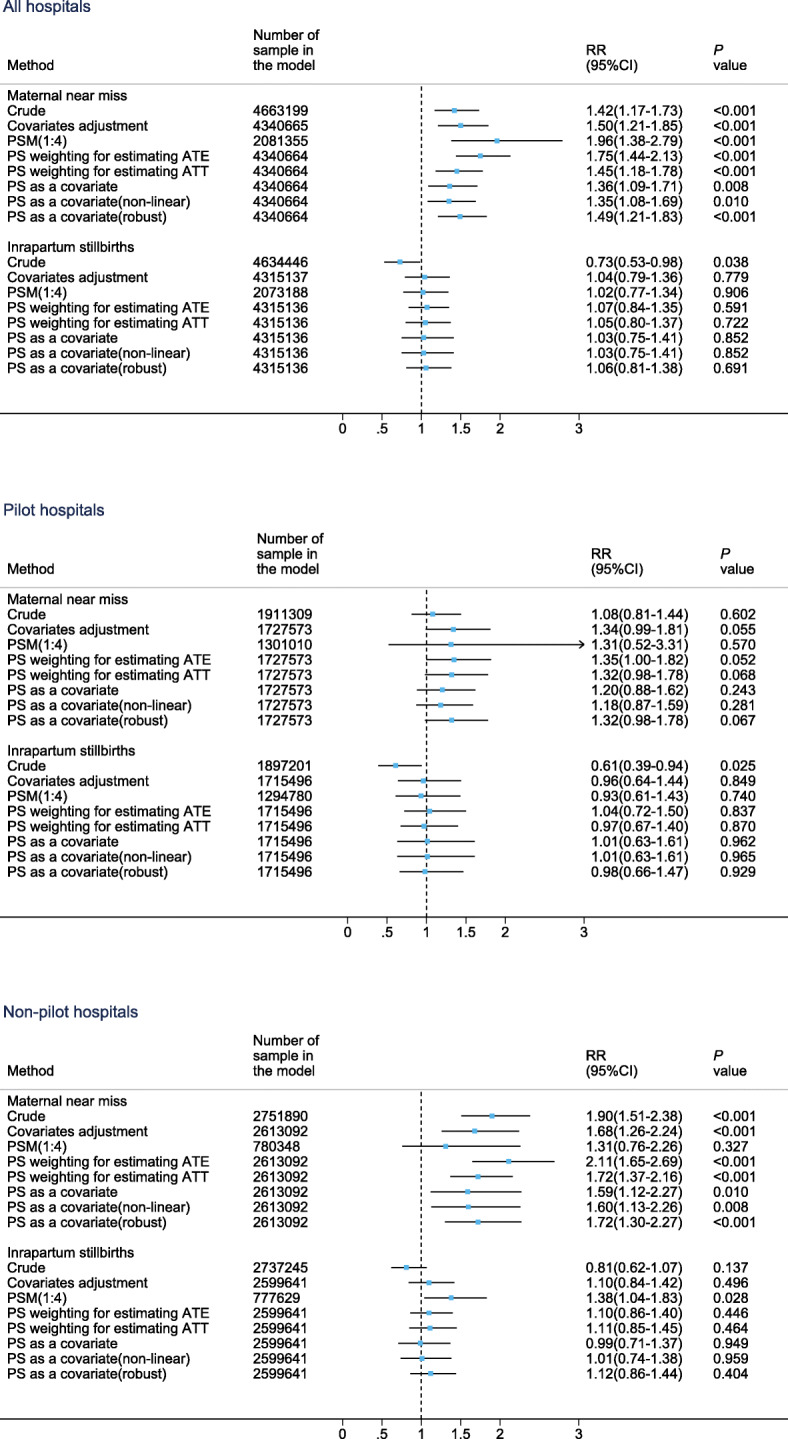
Results: Over the study period, 620,851 of 6,023,046 women underwent vaginal delivery with NA. The estimated national NA rates increased from 8.4% in 2012 to 16.7% in 2019. Most provinces experienced the same rapid rise during this period. The national pilot policy accelerated the rise of the rates. No differences were observed between women with NA and without any analgesia in the incidence of uterine atony, placental retention, intrapartum stillbirths and 1- and 5-min Apgar scores lower than 7. However, women with NA had higher incidences of genital tract trauma (adjusted relative risk (aRR) 1.53, 95% confidence interval (CI) 1.04-2.26) and maternal near miss (aRR 1.35, 95% CI 1.08-1.69), only in hospitals which were not covered by the national pilot policy and usually lack of sufficient equipment and personnel.
Conclusions: The national policy can effectively increase the NA rate. However, as genital tract trauma and maternal near miss may increase in low-resource hospitals, but not in high-resource hospitals, further study is required to identify the reasons.
Keywords: Bayesian multilevel model; China; Interrupted time-series analysis; Intervention; Labour neuraxial analgesia; Maternal near miss; Propensity score.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Qu Y. Necessity of promoting for labor analgesia technology and the challenges facing. Int J Anesth Resu. 2008;29(6):574–577.
-
- National Health Commission of the People’s Republic of China . Opinions on strengthening and improving Anaesthesia Medical Service [in Chinese] 2018.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
