

May-Thurner syndrome, a diagnosis to consider in young males with no risk factors: a case report and review of the literature
- PMID: 33736685
- PMCID: PMC7977182
- DOI: 10.1186/s13256-021-02730-8
May-Thurner syndrome, a diagnosis to consider in young males with no risk factors: a case report and review of the literature
Erratum in
-
Correction to: May-Thurner syndrome, a diagnosis to consider in young males with no risk factors: a case report and review of the literature.J Med Case Rep. 2021 Nov 26;15(1):571. doi: 10.1186/s13256-021-03195-5. J Med Case Rep. 2021. PMID: 34836542 Free PMC article. No abstract available.
Abstract
Background: May-Thurner syndrome is an anatomical condition characterized by compression of the left common iliac vein by the right common iliac artery, causing venous outflow obstruction. It is an uncommon cause of deep vein thrombosis and is more prevalent among women. This paper highlights the importance of considering May-Thurner syndrome in young males without risk factors presenting with left lower limb pain, as endovascular treatment may be required.
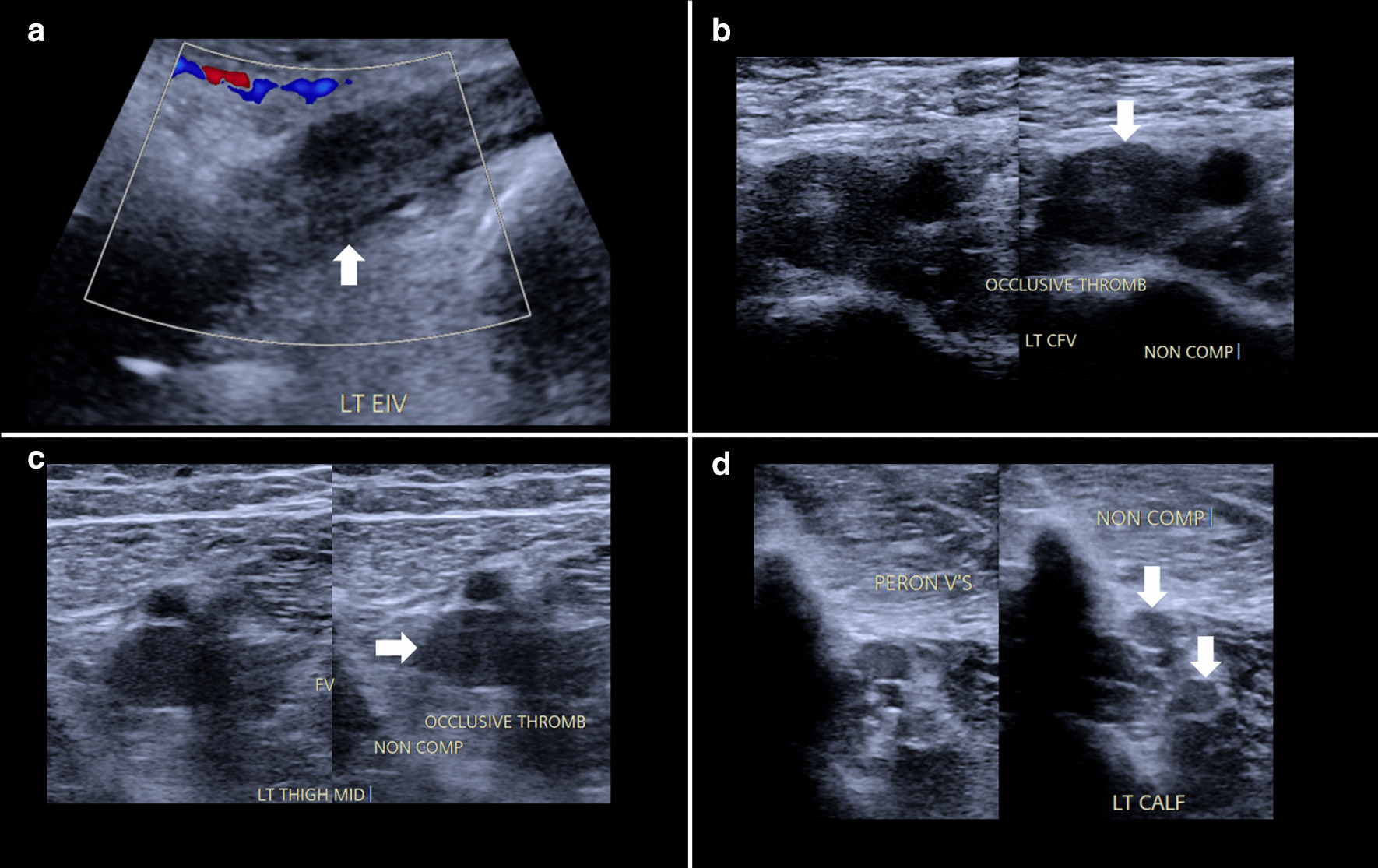
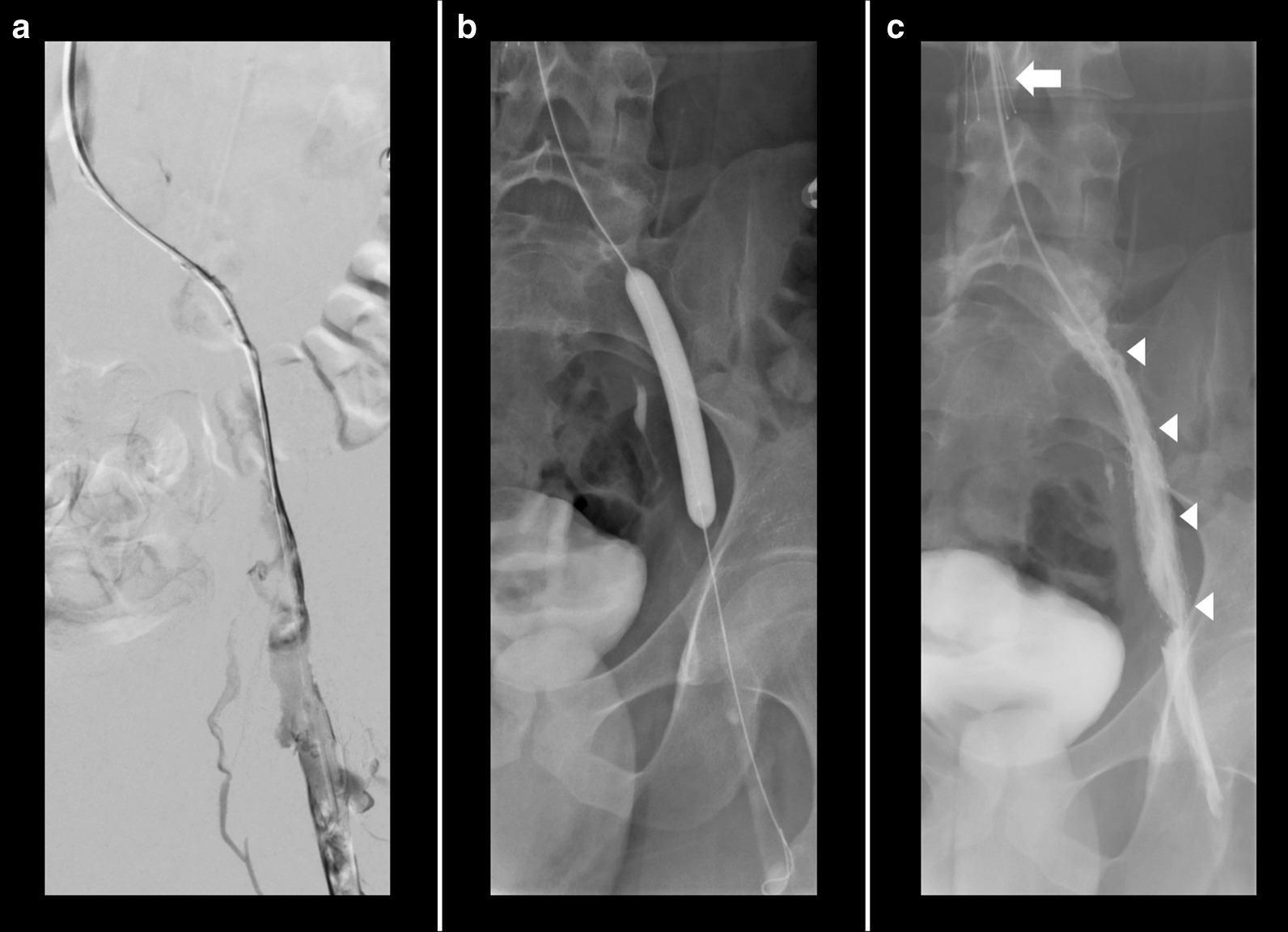
Case presentation: A 23 year-old Caucasian male presented with a 1-week history of left lower limb pain, edema, and pallor. He was found to have an unprovoked deep vein thrombosis on Doppler ultrasound involving the left fibular, soleus, gastrocnemius, popliteal, femoral, common femoral, and external iliac veins. A heparin infusion was commenced as the initial treatment for deep vein thrombosis. Further investigation with computer tomography pulmonary angiogram and computer tomography venography of the abdomen and pelvis showed bilateral pulmonary emboli and left common iliac vein compression with left common, internal, and external iliac vein thrombosis. He was diagnosed with May-Thurner syndrome despite having no risk factors. A retrievable Cook Celect Platinum inferior vena cava filter was placed, and thrombus of the left common femoral, external, and common iliac veins was treated successfully with AngioJet thrombectomy, thrombolysis using 200,000 units of urokinase, angioplasty and stenting using two Cook Zilver Vena venous self-expanding stents. Therapeutic enoxaparin was commenced on discharge. His filter was removed after 10 weeks. Hematological follow-up 4 months later showed an overall negative thrombophilia screen, and anticoagulation was switched to apixaban. He has had no recurrent thrombosis.
Conclusions: Clinicians should have a low threshold to investigate for May-Thurner syndrome in patients with left lower limb venous thrombotic events regardless of risk factors, as endovascular treatment may be required to minimize the long-term sequelae of deep vein thrombosis. Duplex ultrasound can be used initially for diagnosis, and computer tomography venography used subsequently if the common iliac vein is not visualized on ultrasound. Endovascular treatment is preferred over anticoagulation alone, especially in otherwise fit patients presenting early, the aim being to reduce the chances of chronic venous hypertension in the lower limb.
Keywords: Case report; Computer tomography venography; Deep vein thrombosis; Endovascular; Left common iliac vein; May–Thurner syndrome; Risk factors; Stent; Ultrasound; Venous hypertension.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
