

Outcomes of Premature Ventricular Contraction-Cardiomyopathy in the Veteran Population: A Secondary Analysis of the CHF-STAT Study
- PMID: 33736756
- PMCID: PMC9188841
- DOI: 10.1016/j.jacep.2020.08.028
Outcomes of Premature Ventricular Contraction-Cardiomyopathy in the Veteran Population: A Secondary Analysis of the CHF-STAT Study
Abstract
Objectives: This study sought to assess the rate and outcomes of premature ventricular contractions (PVC)-cardiomyopathy from the CHF-STAT (Survival Trial of Antiarrhythmic Therapy in Congestive Heart Failure) trial, a population with cardiomyopathy (left ventricular [LV] ejection fraction of <40%) and frequent PVCs (>10 PVCs per hour).
Background: PVCs are associated with heart failure and PVC-cardiomyopathy. The prevalence of PVC-cardiomyopathy and outcome benefits of PVC suppression are not clear.
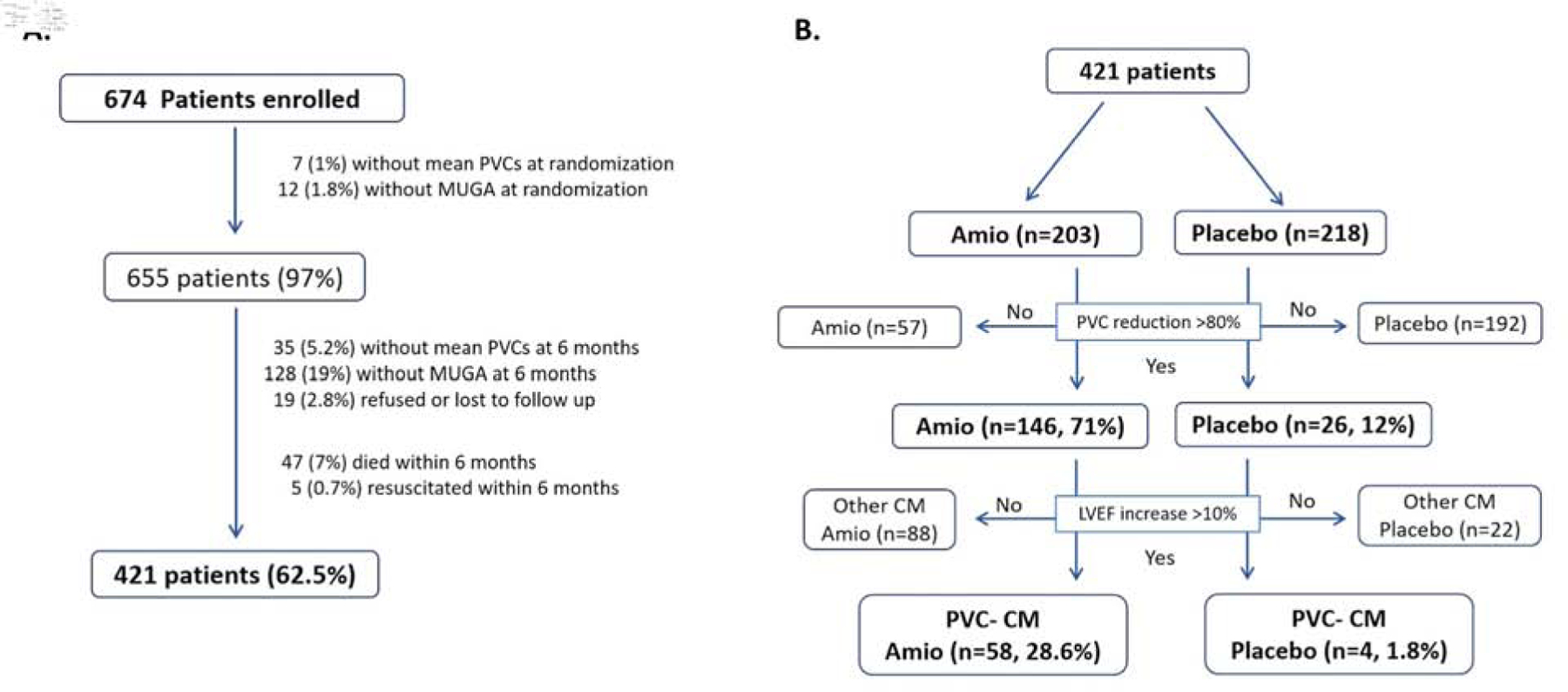
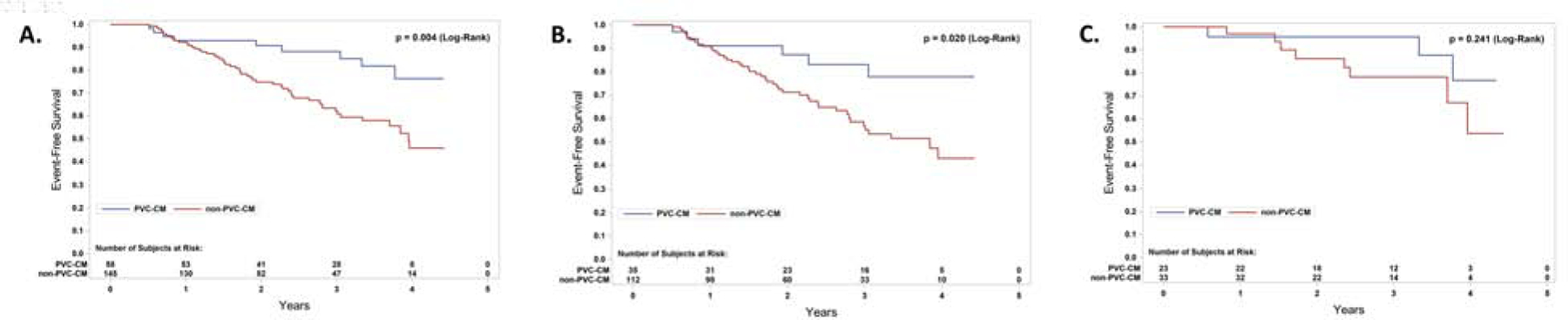
Methods: A secondary analysis of the CHF-STAT study was performed to compare the rate of successful PVC suppression (≥80% PVC reduction), LV recovery (defined as improvement in LV ejection fraction of ≥10% points), and PVC-cardiomyopathy between amiodarone and placebo groups at 6 months. PVC-cardiomyopathy was defined if both PVC reduction of ≥80% and LV ejection fraction improvement of ≥10% were present at 6 months. Cardiac events (death or resuscitated cardiac arrest) were compared between PVC-cardiomyopathy versus non-PVC-cardiomyopathy during a 5-year follow-up.
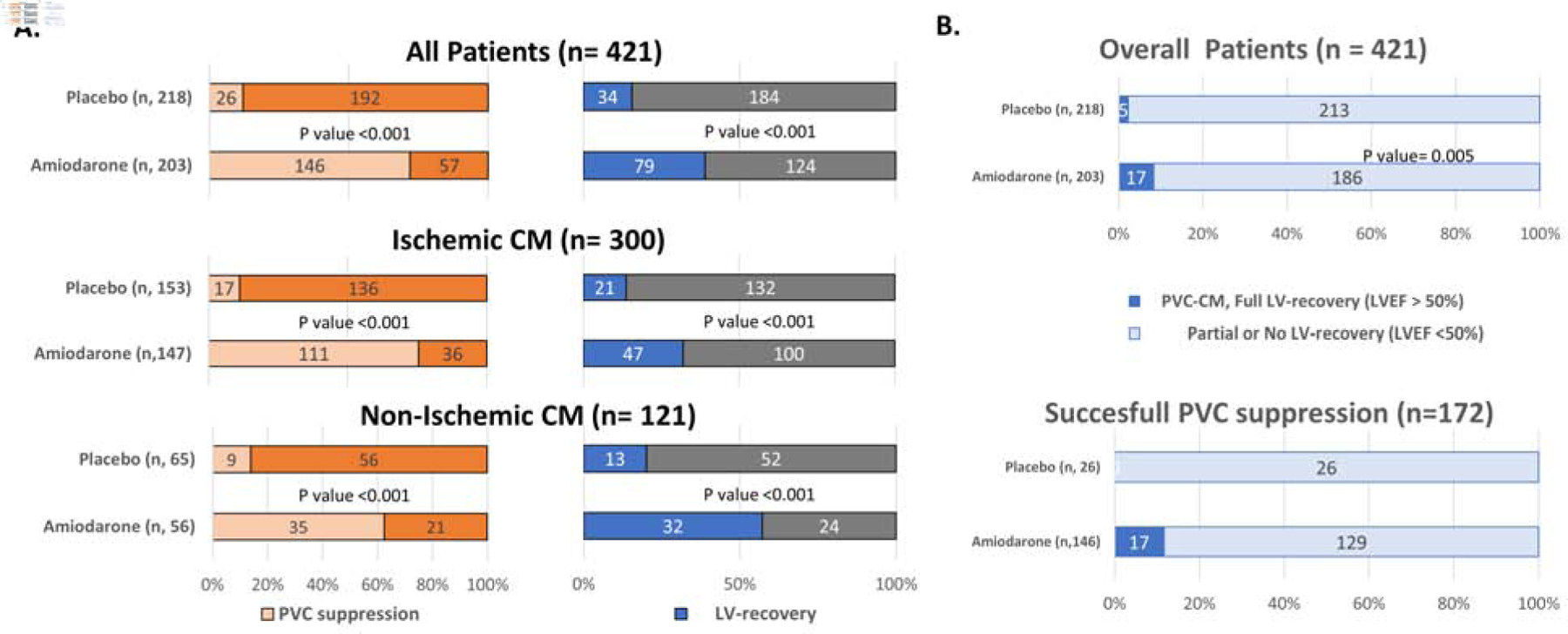
Results: The rates of successful PVC suppression and LV recovery were significantly higher in the amiodarone (72% and 39%, respectively) when compared to the placebo group (12% and 16%, respectively; p < 0.001), regardless of cardiomyopathy etiology. PVC-cardiomyopathy was present in 29% and 1.8% of patients in the amiodarone and placebo groups, respectively (p < 0.001). Similar PVC-cardiomyopathy rates were found in ischemic (24% amiodarone vs. 2% placebo; p < 0.001) and nonischemic populations (41% amiodarone vs. 1.5% placebo; p < 0.001). Death and resuscitated cardiac arrest were significantly lower in patients with PVC-cardiomyopathy and those treated with amiodarone.
Conclusions: The overall prevalence of PVC-cardiomyopathy in the CHF-STAT study was significant regardless of ischemic substrate (29%, overall population; 41%, nonischemic cardiomyopathy). Treatment of PVC-cardiomyopathy with amiodarone is likely to improve survival in this high-risk population.
Keywords: LV systolic dysfunction; amiodarone; antiarrhythmics; cardiomyopathy; premature ventricular contractions.
Published by Elsevier Inc.
Conflict of interest statement
FUNDING SUPPORT AND AUTHOR DISCLOSURES Supported by 1R01HL139874-01 (Principal Investigator: Dr. Huizar), 5R34HL138110-02 (Principal Investigator: Dr. Huizar). Dr. Huizar has received research support from Abbott. Dr. Kaszala has received research support from Boston Scientific and Abbott. Dr. Tan has received research support from Boston Scientific, MDT, and Biotronik. Dr. Ellenbogen has received research support from Boston Scientific, Biosense Webster, MDT, Abbott, and the National Institutes of Health; has served as a consultant for Boston Scientific, Abbott, Atricure, and Medtronic; and has received honoraria from MDT, Boston Scientific, Biotronik, Biosense Webster, and Atricure. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures

Comment in
-
Can the Past Re-Shape the Future?: New Insights Into PVC-Mediated Cardiomyopathy From the CHF-STAT Trial and the Retelling of a Familiar Story.JACC Clin Electrophysiol. 2021 Mar;7(3):391-394. doi: 10.1016/j.jacep.2020.11.020. JACC Clin Electrophysiol. 2021. PMID: 33736757 No abstract available.
References
-
- Baman TS, Lange DC, Ilg KJ et al. Relationship between burden of premature ventricular complexes and left ventricular function. Heart Rhythm 2010;7:865–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
