

Type 2 Diabetes and Cancer: An Umbrella Review of Observational and Mendelian Randomization Studies
- PMID: 33737302
- PMCID: PMC9398112
- DOI: 10.1158/1055-9965.EPI-20-1245
Type 2 Diabetes and Cancer: An Umbrella Review of Observational and Mendelian Randomization Studies
Abstract
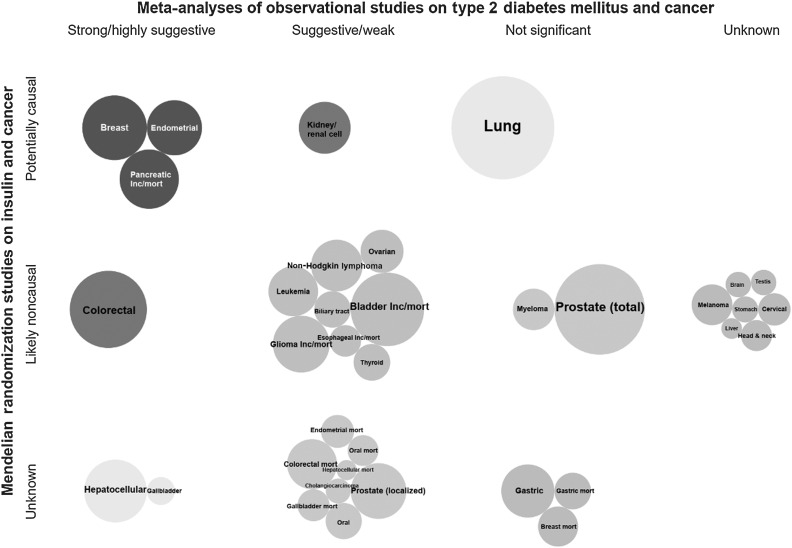
Background: Type 2 diabetes mellitus (T2DM) has been associated with an increased risk of developing several common cancers, but it is unclear whether this association is causal. We aimed to summarize the evidence on T2DM and cancer and evaluate the validity of associations from both observational and Mendelian randomization (MR) studies.
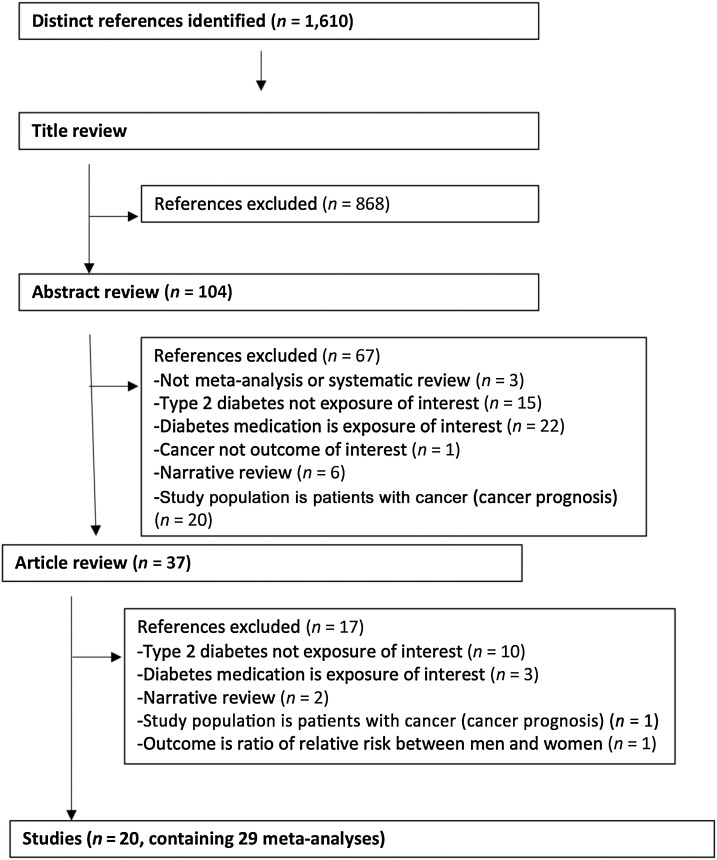
Methods: We performed an umbrella review of the evidence across meta-analyses of observational studies that examined associations of T2DM with risk of developing or dying from site-specific cancers, and MR studies that explored the potential causal association of T2DM and associated biomarkers with cancer risk.
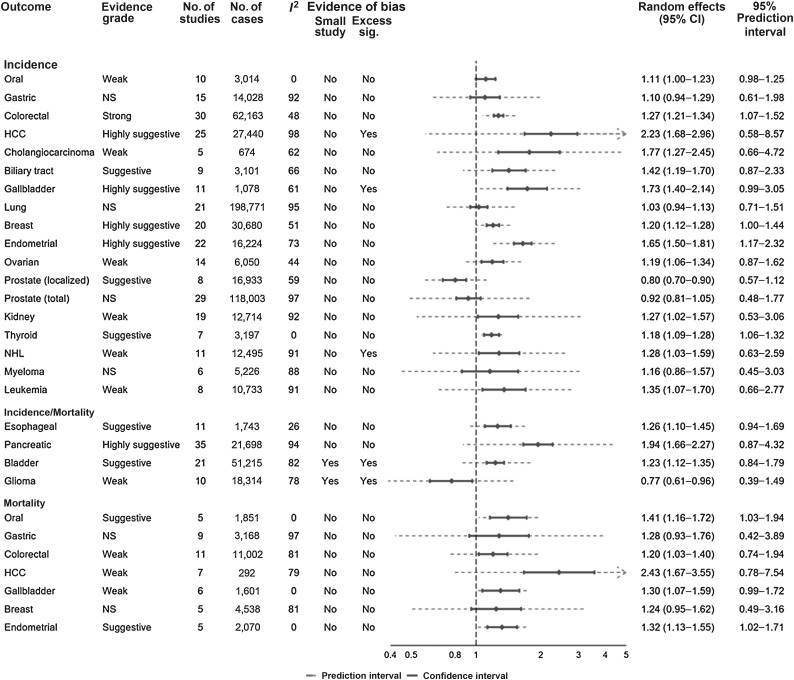
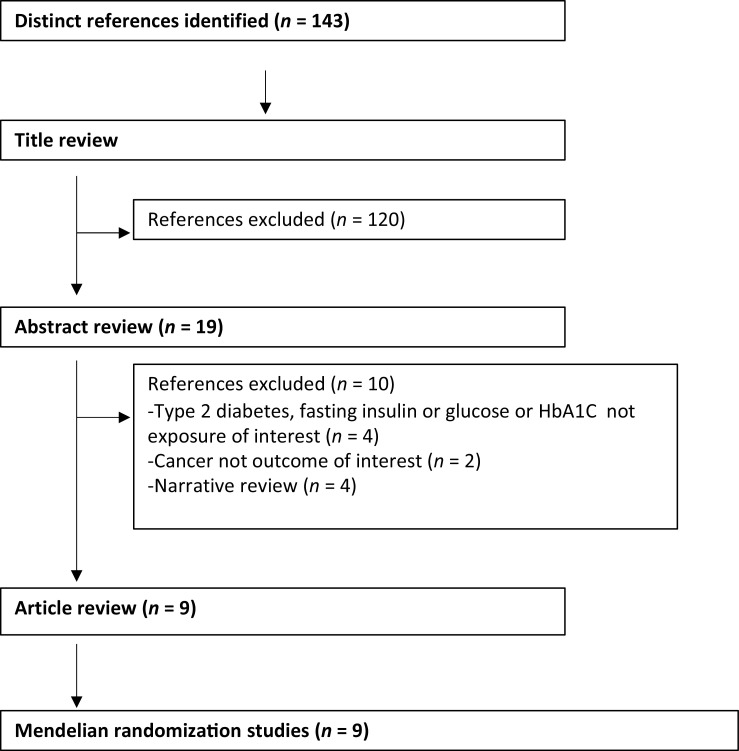
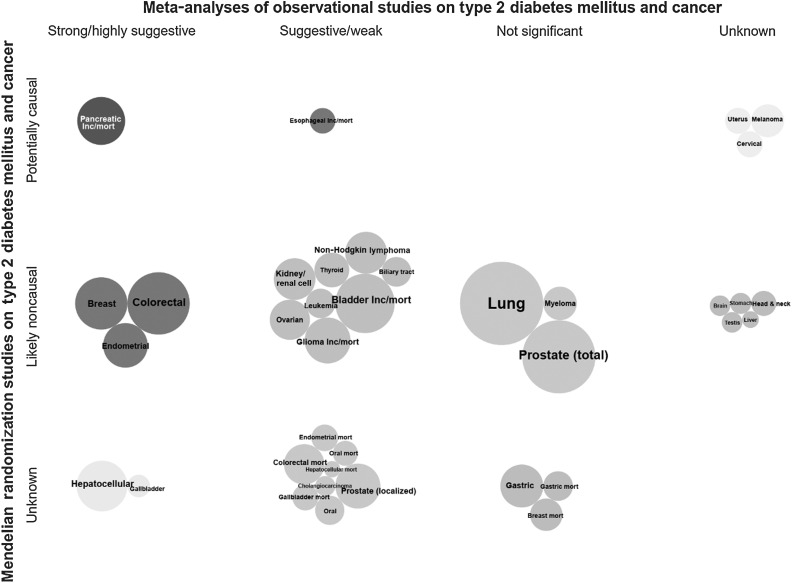
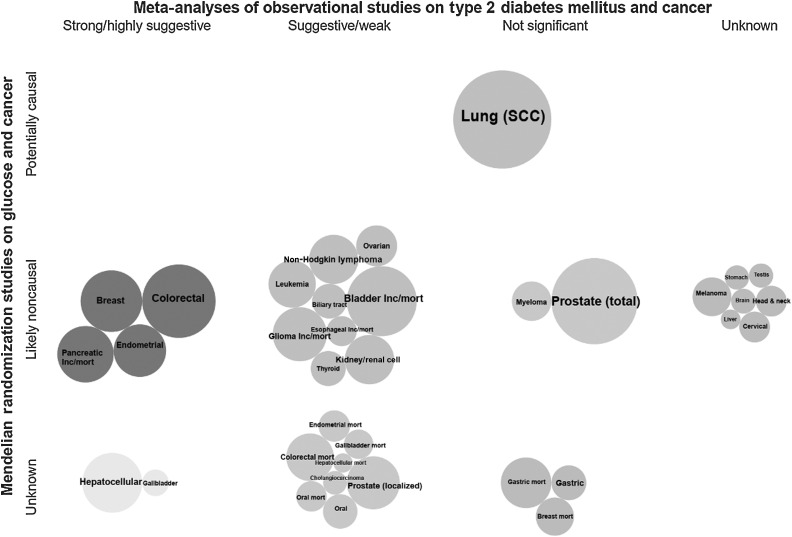
Results: We identified eligible observational meta-analyses that assessed associations between T2DM and cancer incidence for 18 cancer sites, cancer mortality for seven sites, and cancer incidence or mortality for four sites. Positive associations between T2DM and six cancers reached strong or highly suggestive evidence. We found eight MR studies assessing the association of genetically predicted T2DM and seven and eight studies assessing the association of genetically predicted fasting insulin or fasting glucose concentrations, respectively, upon site-specific cancers. Positive associations were found between genetically predicted T2DM and fasting insulin and risk of six cancers. There was no association between genetically predicted fasting plasma glucose and cancer except for squamous cell lung carcinoma.
Conclusions: We found robust observational evidence for the association between T2DM and colorectal, hepatocellular, gallbladder, breast, endometrial, and pancreatic cancers.
Impact: Potential causal associations were identified for genetically predicted T2DM and fasting insulin concentrations and risk of endometrial, pancreas, kidney, breast, lung, and cervical cancers.
©2021 American Association for Cancer Research.
Figures
Comment in
- Cancer Epidemiol Biomarkers Prev. 30:1033.
References
-
- Genuth S, Eastman R, Kahn R, Klein R, Lachin J, Lebovitz H, et al. Implications of the United kingdom prospective diabetes study. Diabetes Care 2003;26:S28–32. - PubMed
-
- National Institute for Health and Care Excellence. NICE Guidelines Clinical Guidelines 66—TYPE 2 diabetes. Available from:https://www.nice.org.uk/guidance/cg66. Accessed 5 Aug2015.
-
- Tsilidis KK, Kasimis JC, Lopez DS, Ntzani EE, Ioannidis JPA. Type 2 diabetes and cancer: umbrella review of meta-analyses of observational studies. BMJ 2015;350:g7607. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
