

Vagus nerve stimulation activates two distinct neuroimmune circuits converging in the spleen to protect mice from kidney injury
- PMID: 33737395
- PMCID: PMC7999957
- DOI: 10.1073/pnas.2021758118
Vagus nerve stimulation activates two distinct neuroimmune circuits converging in the spleen to protect mice from kidney injury
Abstract
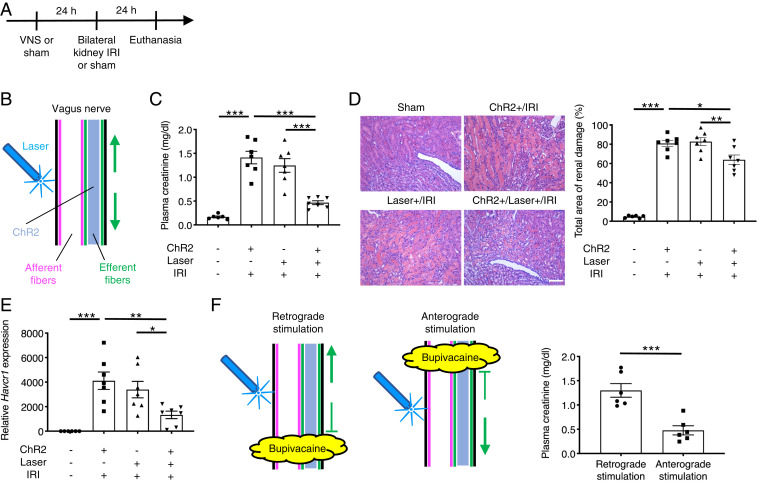
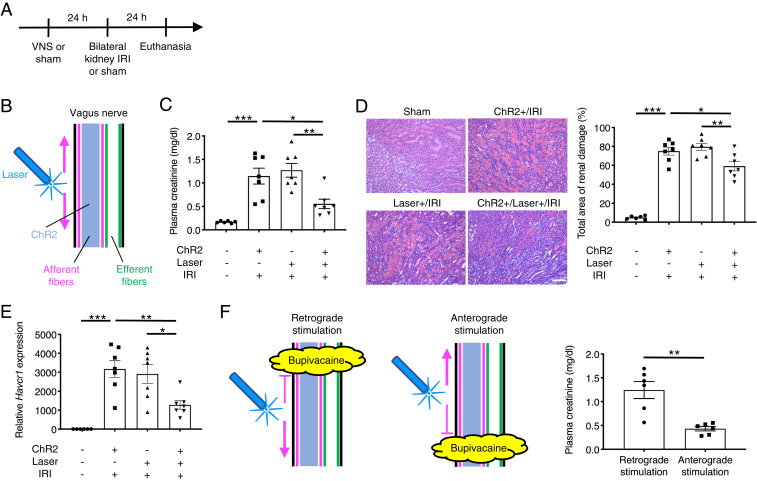
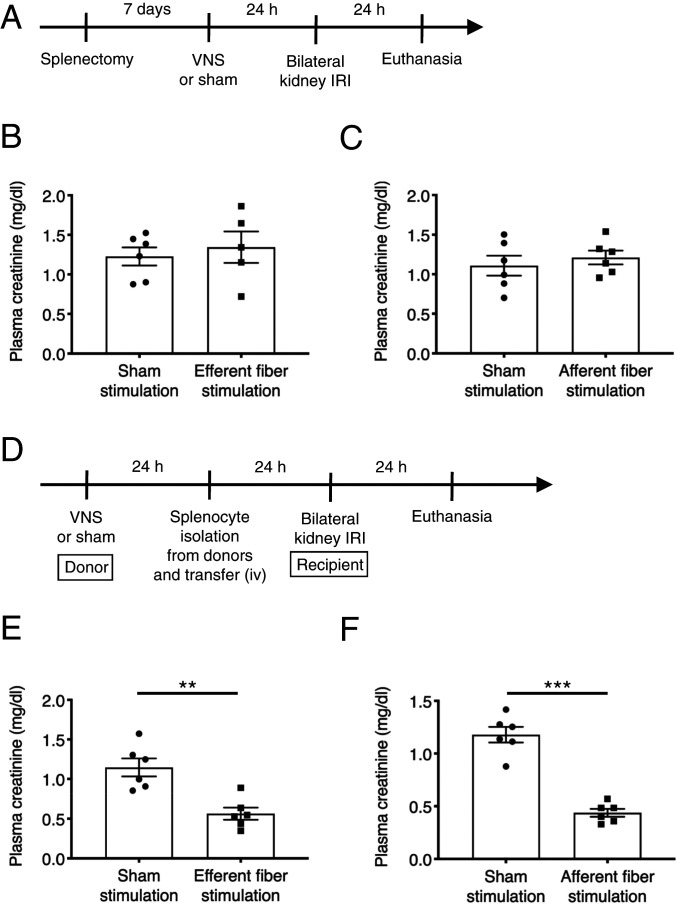
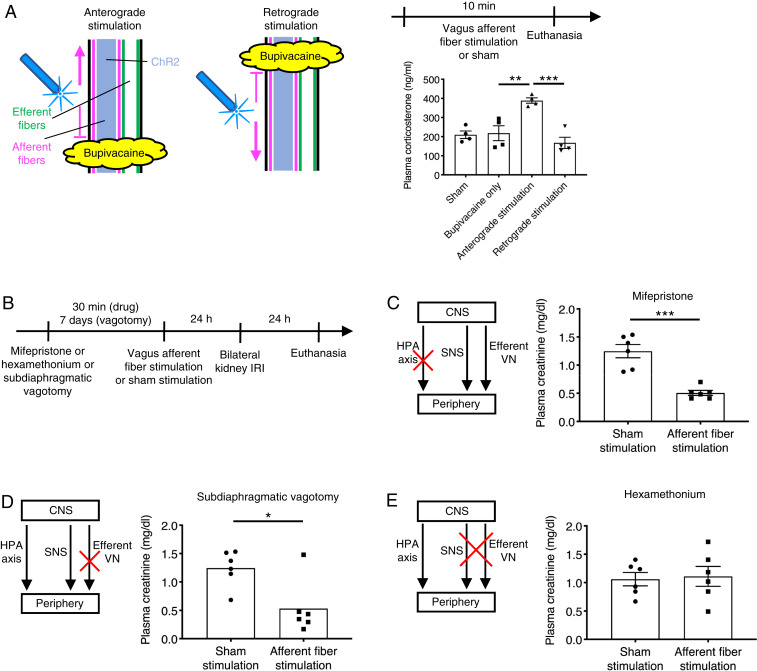
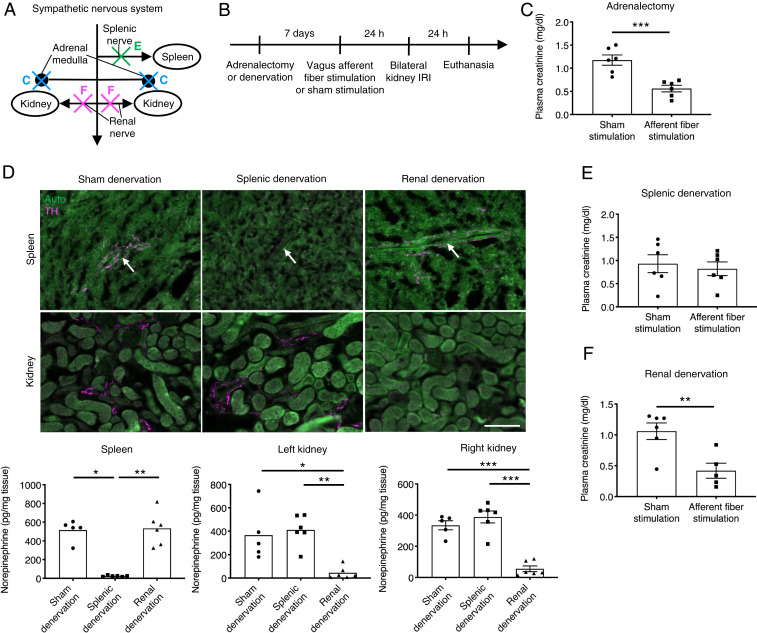
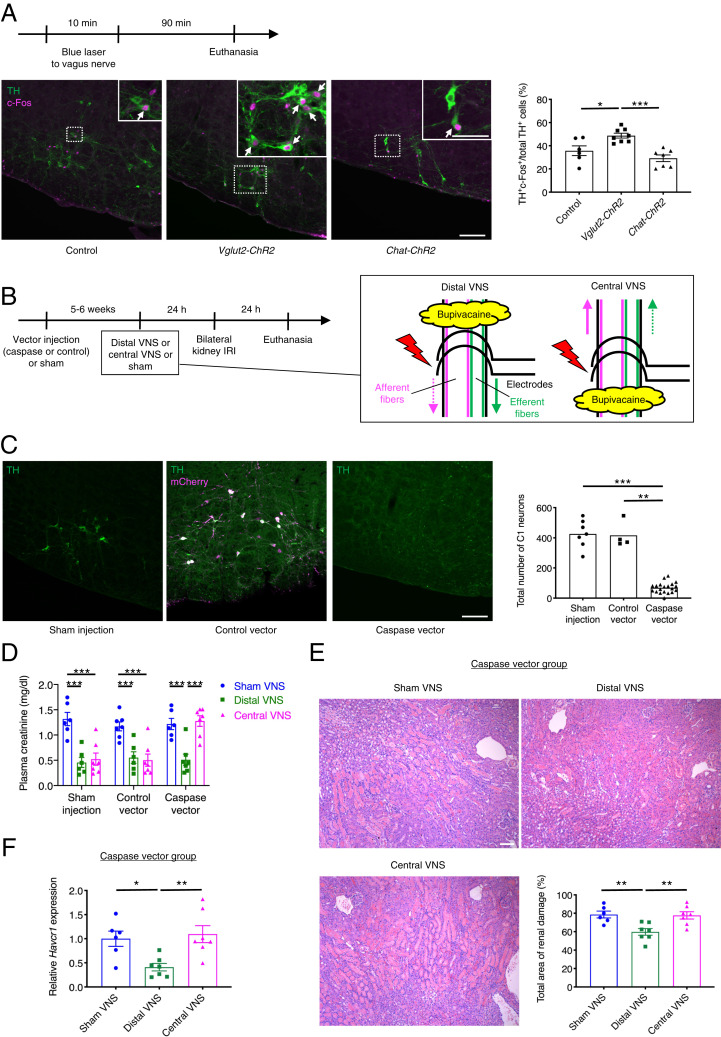
Acute kidney injury is highly prevalent and associated with high morbidity and mortality, and there are no approved drugs for its prevention and treatment. Vagus nerve stimulation (VNS) alleviates inflammatory diseases including kidney disease; however, neural circuits involved in VNS-induced tissue protection remain poorly understood. The vagus nerve, a heterogeneous group of neural fibers, innervates numerous organs. VNS broadly stimulates these fibers without specificity. We used optogenetics to selectively stimulate vagus efferent or afferent fibers. Anterograde efferent fiber stimulation or anterograde (centripetal) sensory afferent fiber stimulation both conferred kidney protection from ischemia-reperfusion injury. We identified the C1 neurons-sympathetic nervous system-splenic nerve-spleen-kidney axis as the downstream pathway of vagus afferent fiber stimulation. Our study provides a map of the neural circuits important for kidney protection induced by VNS, which is critical for the safe and effective clinical application of VNS for protection from acute kidney injury.
Keywords: acute kidney injury; neuroimmune interactions; sympathetic nervous system; vagus nerve stimulation.
Conflict of interest statement
The authors declare no competing interest.
Figures
References
-
- Ronco C., Bellomo R., Kellum J. A., Acute kidney injury. Lancet 394, 1949–1964 (2019). - PubMed
-
- Levey A. S., James M. T., Acute kidney injury. Ann. Intern. Med. 167, ITC66–ITC80 (2017). - PubMed
-
- Webster A. C., Nagler E. V., Morton R. L., Masson P., Chronic kidney disease. Lancet 389, 1238–1252 (2017). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
