

Evaluating access to health and care services during lockdown by the COVID-19 survey in five UK national longitudinal studies
- PMID: 33737441
- PMCID: PMC7978270
- DOI: 10.1136/bmjopen-2020-045813
Evaluating access to health and care services during lockdown by the COVID-19 survey in five UK national longitudinal studies
Abstract
Objective: Access to health services and adequate care is influenced by sex, ethnicity, socioeconomic position (SEP) and the burden of comorbidities. Our study aimed to assess whether the COVID-19 pandemic further deepened these already existing health inequalities.
Design: Cross-sectional study.
Setting: Data were collected from five longitudinal age-homogenous British cohorts (born in 2000-2002, 1989-1990, 1970, 1958 and 1946).
Participants: A web survey was sent to the cohorts. Anybody who responded to the survey was included, resulting in 14 891 eligible participants.
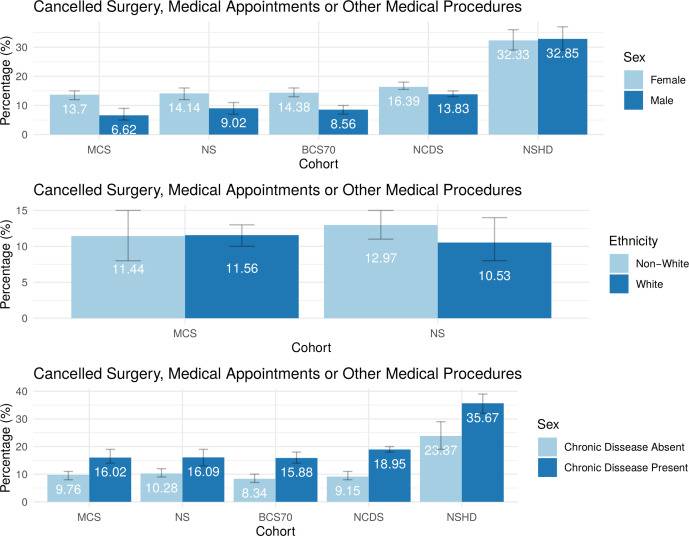
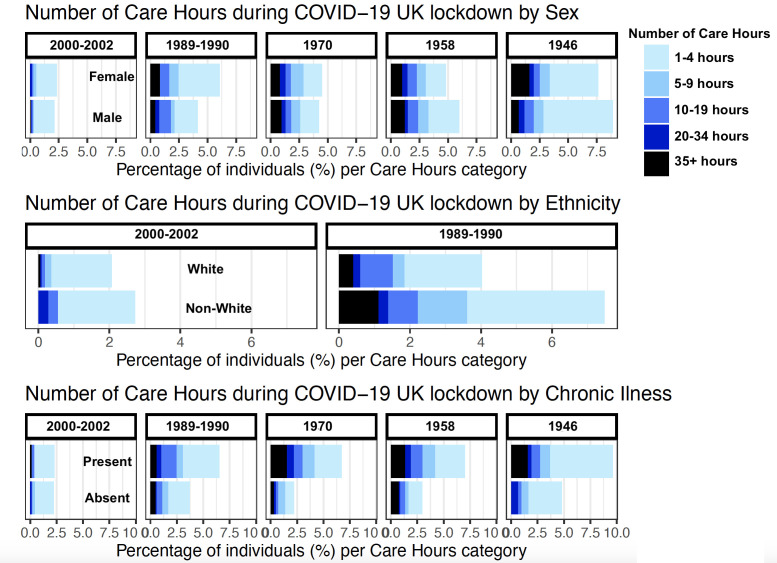
Main outcomes measured: The survey provided data on cancelled surgical or medical appointments, and the number of care hours received in a week during the first UK COVID-19 national lockdown.
Interventions: Using binary or ordered logistic regression, we evaluated whether these outcomes differed by sex, ethnicity, SEP and having a chronic illness. Adjustment was made for study design, non-response weights, psychological distress, presence of children or adolescents in the household, COVID-19 infection, key worker status, and whether participants had received a shielding letter. Meta-analyses were performed across the cohorts, and meta-regression was used to evaluate the effect of age as a moderator.
Results: Women (OR 1.40, 95% CI 1.27 to 1.55) and those with a chronic illness (OR 1.84, 95% CI 1.65 to 2.05) experienced significantly more cancellations during lockdown (all p<0.0001). Ethnic minorities and those with a chronic illness required a higher number of care hours during the lockdown (both OR≈2.00, all p<0.002). SEP was not associated with cancellation or care hours. Age was not independently associated with either outcome in the meta-regression.
Conclusion: The UK government's lockdown approach during the COVID-19 pandemic appears to have deepened existing health inequalities, impacting predominantly women, ethnic minorities and those with chronic illnesses. Public health authorities need to implement urgent policies to ensure equitable access to health and care for all in preparation for a fourthwave.
Keywords: epidemiology; public health; quality in health care.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical