

Tumours of the odontoid peg revisited
- PMID: 33737770
- PMCID: PMC7954168
- DOI: 10.4103/ijri.IJRI_363_20
Tumours of the odontoid peg revisited
Abstract
Introduction: Tumours of the odontoid peg are rare but can potentially cause significant morbidity and mortality.
Methods: A retrospective review of oncology and radiology database of tertiary orthopaedic oncology centre for all lesions affecting the odontoid peg over the last 12 years was performed.
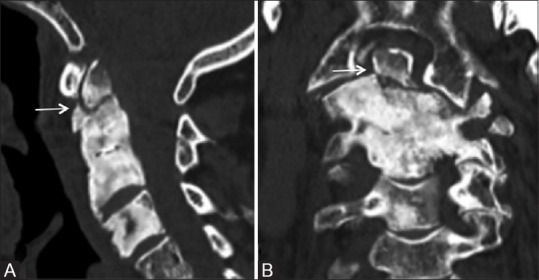
Results: We identified a total of 15 tumours involving the odontoid peg, majority being malignant. Myeloma was the most common tumour.
Conclusion: Tumours of the odontoid peg are rare. Spinal surgeons and Radiologists need to be aware of them.
Keywords: Odonotid; imaging; tumour.
Copyright: © 2021 Indian Journal of Radiology and Imaging.
Conflict of interest statement
There are no conflicts of interest.
Figures







Similar articles
-
Management of C2 odontoid peg fragility fractures - A UK survey of spinal surgeons.Injury. 2022 Mar;53(3):1057-1061. doi: 10.1016/j.injury.2021.09.057. Epub 2021 Oct 1. Injury. 2022. PMID: 34635337
-
Survival analysis of elderly patients with a fracture of the odontoid peg.Bone Joint J. 2014 Jan;96-B(1):88-93. doi: 10.1302/0301-620X.96B1.32024. Bone Joint J. 2014. PMID: 24395317
-
The three-dimensional morphometry of the odontoid peg and its impact on ventral screw osteosynthesis.Bone Joint J. 2013 Apr;95-B(4):536-42. doi: 10.1302/0301-620X.95B4.30949. Bone Joint J. 2013. PMID: 23539707
-
Conservative Management of Odontoid Peg Fractures, long term follow up.J Clin Orthop Trauma. 2017 Apr-Jun;8(2):103-106. doi: 10.1016/j.jcot.2017.06.003. Epub 2017 Jun 4. J Clin Orthop Trauma. 2017. PMID: 28720985 Free PMC article. Review.
-
Musculoskeletal tumours and tumour-like conditions: common and avoidable pitfalls at imaging in patients with known or suspected cancer: Part B: malignant mimics of benign tumours.Int Orthop. 2013 May;37(5):877-82. doi: 10.1007/s00264-013-1824-6. Epub 2013 Feb 17. Int Orthop. 2013. PMID: 23417556 Free PMC article. Review.
Cited by
-
Challenges in Diagnosis and Management of Atlantoaxial Tuberculosis: A Case Report.Medicina (Kaunas). 2025 Jan 26;61(2):224. doi: 10.3390/medicina61020224. Medicina (Kaunas). 2025. PMID: 40005341 Free PMC article.
-
An Unusual Chordoma of the Odontoid Process: A Case Report and Literature Review.J Am Acad Orthop Surg Glob Res Rev. 2022 May 1;6(5):e22.00018. doi: 10.5435/JAAOSGlobal-D-22-00018. J Am Acad Orthop Surg Glob Res Rev. 2022. PMID: 35584249 Free PMC article. Review.
References
-
- Redlund-Johnell I, Pettersson H. Radiographic measurements of thecranio-vertebral region. Designed for evaluation of abnormalities in rheumatoidarthritis. Acta Radiol Diagn (Stockh) 1984;25:23–8. - PubMed
-
- Schweitzer ME, Hodler J, Cervilla V, Resnick D. Craniovertebral junction: Normal anatomy with MR correlation. AJR Am J Roentgenol. 1992;158:1087–90. - PubMed
-
- Bladè J, Fernández de Larrea C, Rosiñol L, Cibeira MT, Jimènez R, Powles R. Soft-tissue plasmacytomas in multiple myeloma: Incidence, mechanisms of extramedullary spread, and treatment approach. J Clin Oncol. 2011;29:3805–12. - PubMed
LinkOut - more resources
Full Text Sources