

Expanded access to multiple sclerosis teleneurology care following the COVID-19 pandemic
- PMID: 33738110
- PMCID: PMC7934057
- DOI: 10.1177/2055217321997467
Expanded access to multiple sclerosis teleneurology care following the COVID-19 pandemic
Abstract
Background: Teleneurology for multiple sclerosis (MS) care was considered feasible, but utilization was limited.
Objective: To describe how the existing teleneurology populations at two academic MS Centers changed during the COVID-19 pandemic.
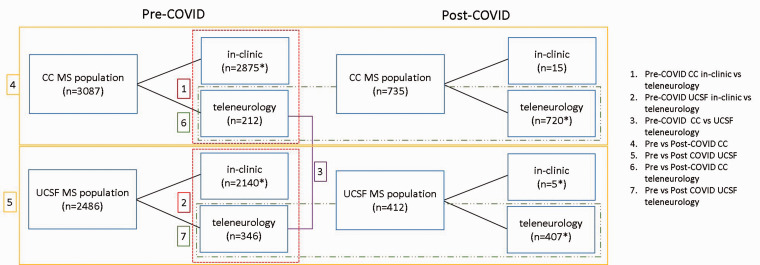
Methods: In this cross-sectional study, we captured all in-person and teleneurology visits at two academic MS Centers between January 2019 and April 2020. We compared group differences between the Centers, and COVID-related changes using T-, chi-squared Kruskal-Wallis and Fisher exact tests.
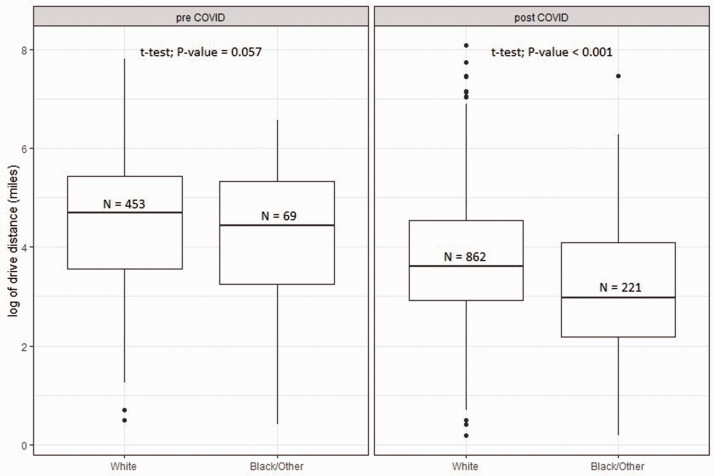
Results: 2268 patients completed 2579 teleneurology visits (mean age 48.3 ± 13.3 years, 72.9% female). Pre-COVID, the Centers' teleneurology populations were similar for age, sex, MS type, and disability level (all p > 0.1), but differed for race (96.5% vs 80.7% white, p ≤ 0.001), MS treatment (49.1% vs 32.1% infusible, p ≤ 0.001), and median distance from Center (72 vs 186 miles, p ≤ 0.001). Post-COVID, both Centers' teleneurology populations had more black (12.7% vs 4.37%, p ≤ 0.001) and local (median 34.5 vs 102 miles, p ≤ 0.001) patients.
Conclusion: Teleneurology visits in 2019 reflected the organizational and local teleneurology reimbursement patterns of our Centers. Our post-COVID-19 changes illustrate the potential for payors and policy to change disparities in access to, or utilization of, remote care. Patients' perception of care quality and value following this shift warrants study.
Keywords: COVID-19; Multiple sclerosis; health disparities; models of care.
© The Author(s) 2021.
Figures
References
-
- Hatcher-Martin JM, Adams JL, Anderson ER, et al. Telemedicine in neurology: Telemedicine Work Group of the American Academy of Neurology update. Neurology 2020; 94(1): 30–38. - PubMed
-
- Tong T, Myers AK, Bissoonauth AA, et al. Identifying the barriers and perceptions of non-Hispanic black and Hispanic/Latino persons with uncontrolled type 2 diabetes for participation in a home telemonitoring feasibility study: a quantitative analysis of those who declined participation, withdrew or were non-adherent. Ethn Health 2020; 25: 485–494. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
