

Segmental Meniscus Allograft Transplantation
- PMID: 33738204
- PMCID: PMC7953169
- DOI: 10.1016/j.eats.2020.10.059
Segmental Meniscus Allograft Transplantation
Abstract
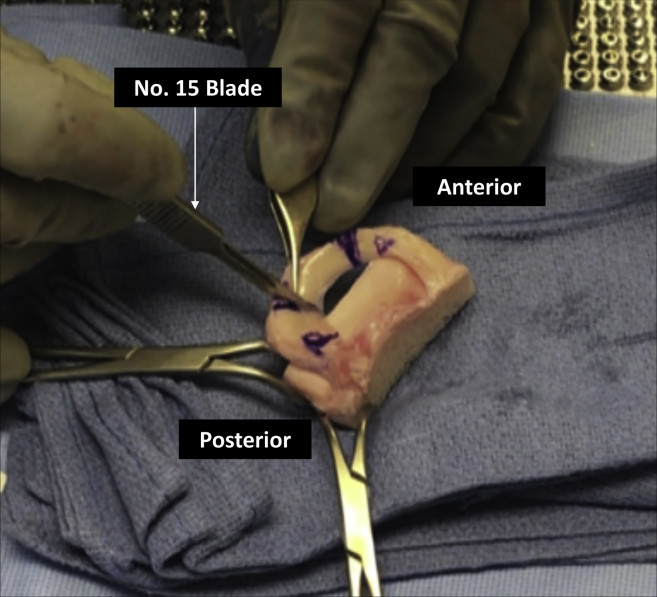
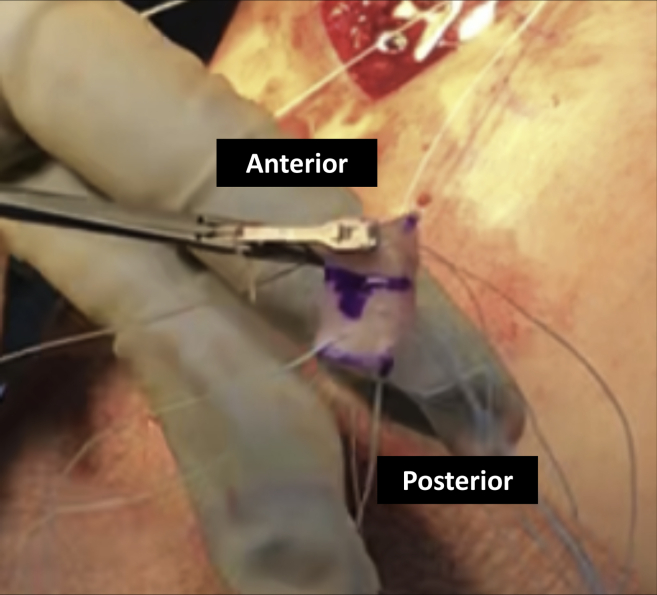
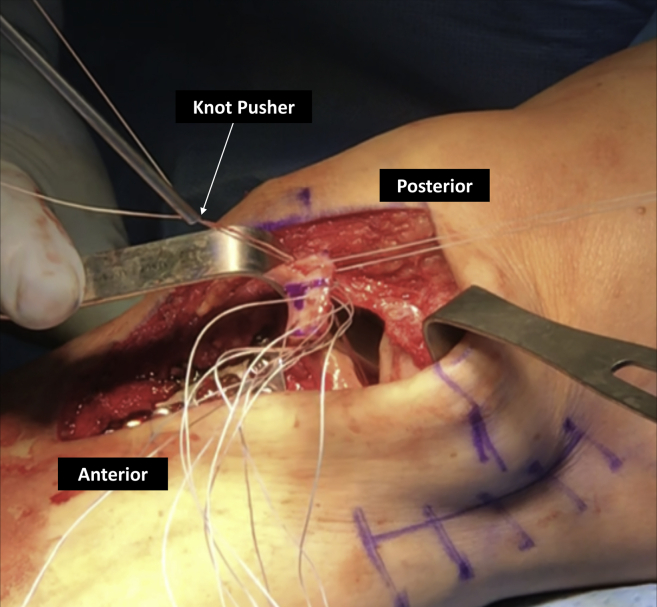
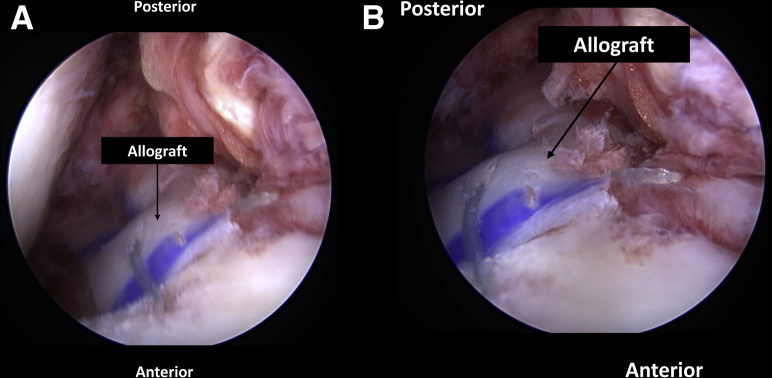
Meniscal tears treated with partial meniscectomies have been shown to significantly increase contract pressures within the tibiofemoral joint, and a complete focal meniscal deficiency may render the entirety of the meniscus functionally incompetent. Although various techniques of meniscal transplantation have been described, these techniques may require the excision of a considerable amount of healthy meniscal tissue. Furthermore, failures continue to frequently occur. Therefore, attempts to restoring normal knee kinematics and biomechanical forces are essential. Segmental meniscus allograft transplantations may offer the advantage of a robust repair by both maintaining knee biomechanics and biology while maximizing preservation of native meniscal tissue. Also, most meniscal deficiency involves only a portion of the meniscus, and thus we developed this technique to segmentally transplant only the deficient portion. The purpose of this Technical Note is to describe a technique of segmental medial meniscus allograft transplantation in a patient with focal medial meniscus deficiency.
Figures

References
-
- Allaire R., Muriuki M., Gilbertson L., Harner C.D. Biomechanical consequences of a tear of the posterior root of the medial meniscus: Similar to total meniscectomy. J Bone Joint Surg Am. 2008;90:1922–1931. - PubMed
-
- Cox J.S., Nye C.E., Schaefer W.W., Woodstein I.J. The degenerative effects of partial and total resection of the medial meniscus in dogs' knees. Clin Orthop Relat Res. 1975;109:178–183. - PubMed
-
- Ichiba A., Kishimoto I. Effects of articular cartilage and meniscus injuries at the time of surgery on osteoarthritic changes after anterior cruciate ligament reconstruction in patients under 40 years old. Arch Orthop Trauma Surg. 2009;129:409–415. - PubMed
-
- Koh J.L., Yi S.J., Ren Y., Zimmerman T.A., Zhang L.Q. Tibiofemoral contact mechanics with horizontal cleavage tear and resection of the medial meniscus in the human knee. J Bone Joint Surg Am. 2016;98:1829–1836. - PubMed
-
- Lee B.S., Bin S.I., Kim J.M. Articular cartilage degenerates after subtotal/total lateral meniscectomy but radiographic arthrosis progression is reduced after meniscal transplantation. Am J Sports Med. 2016;44:159–165. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
