

Multidirectional Shoulder Instability With Circumferential Labral Tear and Bony Reverse Hill Sachs: Treatment with 270° Labral Repair and Fresh Talus Osteochondral Allograft to the Humeral Head
- PMID: 33738215
- PMCID: PMC7953230
- DOI: 10.1016/j.eats.2020.10.068
Multidirectional Shoulder Instability With Circumferential Labral Tear and Bony Reverse Hill Sachs: Treatment with 270° Labral Repair and Fresh Talus Osteochondral Allograft to the Humeral Head
Abstract
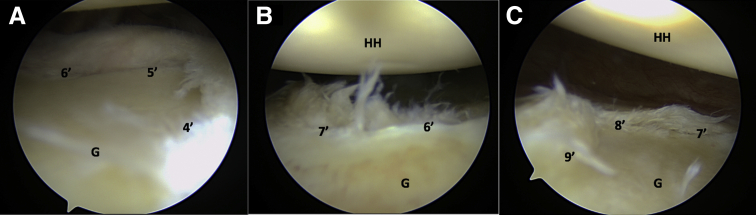
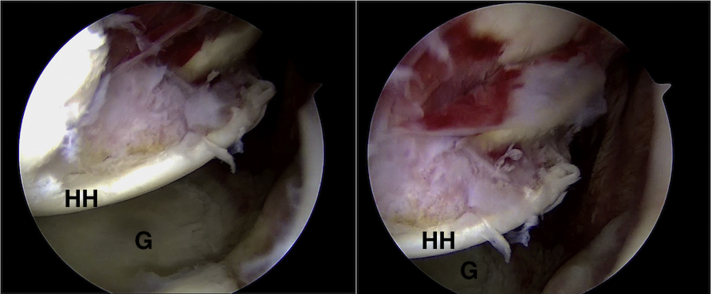
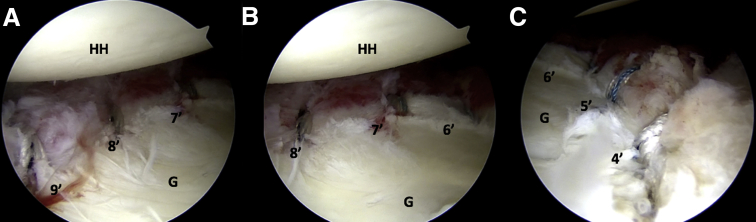
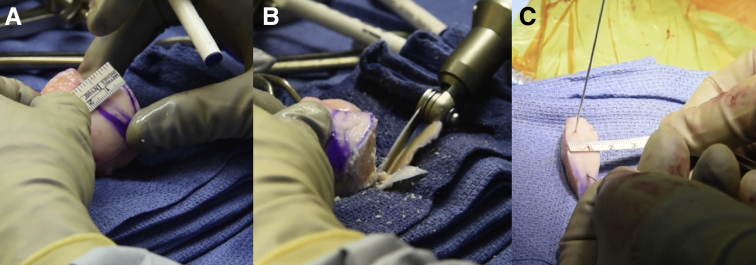
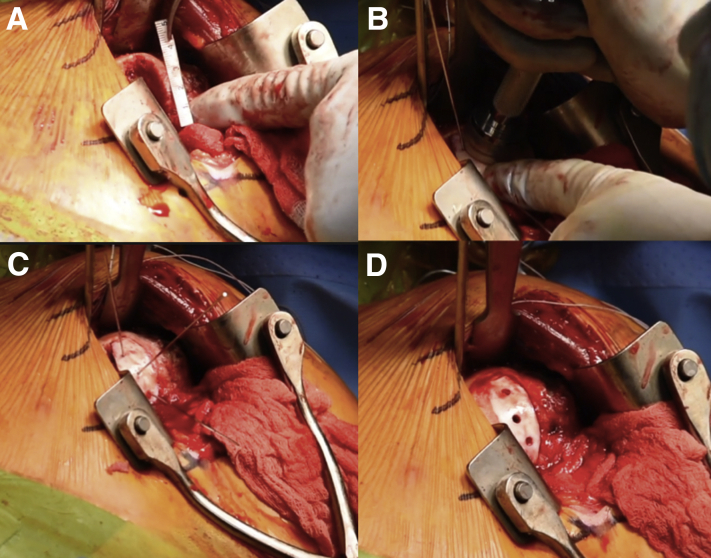
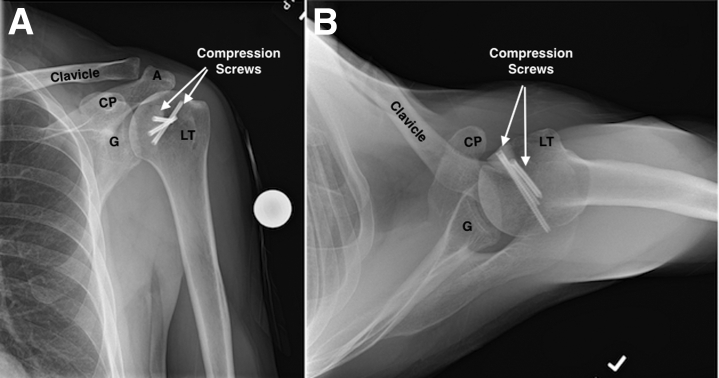
Traumatic posterior dislocations of the shoulder can result in bony defects, labral tears, and cartilage injuries of the glenohumeral joint. Although traditional Hill-Sachs lesions from anterior dislocations are more commonly identified, reverse Hill-Sachs lesions caused by posterior dislocation often leads to recurrent engagement of the humeral head with the glenoid and significantly greater damage to the humeral chondral surface. In severe traumatic cases, concomitant damage of the capsulolabral soft tissues, such as circumferential labral lesions, can lead to chronic shoulder instability and residual glenoid bone loss. These lesions further add to the complexity of managing patients with posterior dislocations of the shoulder because of the challenges of achieving adequate anatomic reduction and tensioning of the capsulolabral junction, while also using a combination of arthroscopic and open-labral repair techniques. In the setting of reverse Hill-Sachs lesions treatment, it is important to address the bony and cartilage defect. The purpose of this Technical Note is to describe our preferred technique for arthroscopic repair of circumferential lesions of the glenoid labrum causing multidirectional instability with concomitant reverse Hill-Sachs Lesion treatment with fresh talus osteochondral allograft.
Figures
Similar articles
-
The effect of a combined glenoid and Hill-Sachs defect on glenohumeral stability: a biomechanical cadaveric study using 3-dimensional modeling of 142 patients.Am J Sports Med. 2015 Jun;43(6):1422-9. doi: 10.1177/0363546515574677. Epub 2015 Mar 20. Am J Sports Med. 2015. PMID: 25794869
-
Concomitant Reverse Hill-Sachs Lesion and Posterior Humeral Avulsion of the Glenohumeral Ligament: Treatment With Fresh Talus Osteochondral Allograft and Arthroscopic Posterior Humeral Avulsion of the Glenohumeral Ligament and Labrum Repair.Arthrosc Tech. 2017 Jul 10;6(4):e987-e995. doi: 10.1016/j.eats.2017.03.012. eCollection 2017 Aug. Arthrosc Tech. 2017. PMID: 28970982 Free PMC article.
-
Anatomic Humeral Head Reconstruction With Fresh Osteochondral Talus Allograft for Recurrent Glenohumeral Instability With Reverse Hill-Sachs Lesion.Arthrosc Tech. 2017 Feb 27;6(1):e255-e261. doi: 10.1016/j.eats.2016.10.017. eCollection 2017 Feb. Arthrosc Tech. 2017. PMID: 28409110 Free PMC article.
-
The Hill-Sachs lesion: diagnosis, classification, and management.J Am Acad Orthop Surg. 2012 Apr;20(4):242-52. doi: 10.5435/JAAOS-20-04-242. J Am Acad Orthop Surg. 2012. PMID: 22474094 Review.
-
Shoulder: Instability.2021 Apr 13. In: Hodler J, Kubik-Huch RA, von Schulthess GK, editors. Musculoskeletal Diseases 2021-2024: Diagnostic Imaging [Internet]. Cham (CH): Springer; 2021. Chapter 1. 2021 Apr 13. In: Hodler J, Kubik-Huch RA, von Schulthess GK, editors. Musculoskeletal Diseases 2021-2024: Diagnostic Imaging [Internet]. Cham (CH): Springer; 2021. Chapter 1. PMID: 33950631 Free Books & Documents. Review.
Cited by
-
Comprehensive Evaluation and Arthroscopic Management of Circumferential Labral Tears Following Traumatic First Time Shoulder Dislocation: A Case Report and Review.J Orthop Case Rep. 2024 Jun;14(6):125-129. doi: 10.13107/jocr.2024.v14.i06.4526. J Orthop Case Rep. 2024. PMID: 38911003 Free PMC article.
-
Knotless Arthroscopic Glenoid Labral Stabilization for a 270° Tear With Concurrent Remplissage in the Lateral Decubitus Position.Arthrosc Tech. 2022 Oct 20;11(11):e1831-e1841. doi: 10.1016/j.eats.2022.06.022. eCollection 2022 Nov. Arthrosc Tech. 2022. PMID: 36457405 Free PMC article.
-
Anatomic Osteochondral Allograft Reconstruction for Concomitant Large Hill-Sachs and Reverse Hill-Sachs Lesions.Arthrosc Tech. 2022 Dec 21;12(1):e53-e57. doi: 10.1016/j.eats.2022.08.057. eCollection 2023 Jan. Arthrosc Tech. 2022. PMID: 36814975 Free PMC article.
References
-
- Owens B.D., Duffey M.L., Nelson B.J., DeBerardino T.M., Taylor D.C., Mountcastle S.B. The Incidence and characteristics of shoulder instability at the United States Military Academy. Am J Sports Med. 2007;35:1168–1173. - PubMed
-
- Kowalsky M.S., Levine W.N. Traumatic posterior glenohumeral dislocation: classification, pathoanatomy, diagnosis, and treatment. Orthop Clin North Am. 2008;39:519–533. - PubMed
-
- Hatzis N., Kaar T.K., Wirth M.A., Rockwood C.A. The often overlooked posterior dislocation of the shoulder. Tex Med. 2001;97:62–67. - PubMed
-
- Robinson C.M., Aderinto J. Posterior shoulder dislocations and fracture-dislocations. J Bone Jt Surg. 2005;87:639–650. - PubMed
-
- Rouleau D.M., Hebert-Davies J. Incidence of associated injury in posterior shoulder dislocation: systematic review of the literature. J Orthop Trauma. 2012;26:246–251. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
