

Impact of a Mortality Prediction Rule for Organizing and Guiding Antimicrobial Stewardship Program Activities
- PMID: 33738318
- PMCID: PMC7953666
- DOI: 10.1093/ofid/ofab056
Impact of a Mortality Prediction Rule for Organizing and Guiding Antimicrobial Stewardship Program Activities
Abstract
Background: Antimicrobial stewardship program (ASP) surveillance at our hospital is supplemented by an internally developed surveillance database. In 2013, the database incorporated a validated, internally developed, prediction rule for patient mortality within 30 days of hospital admission. This study describes the impact of an expanded ASP review in patients at the highest risk for mortality.
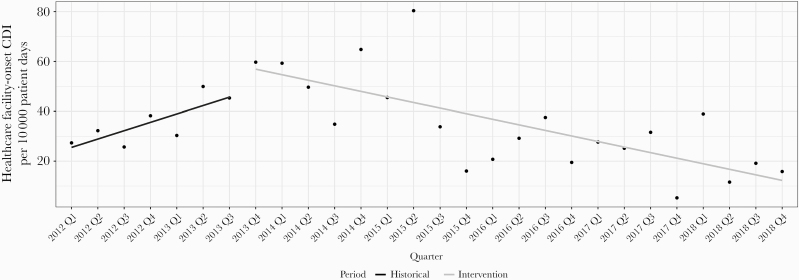
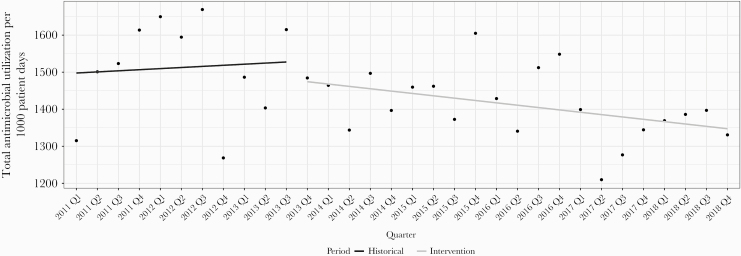
Methods: This retrospective, quasi-experimental study analyzed adults who received antimicrobials with the highest mortality risk score. Study periods were defined as 2011-Q3 2013 (historical group) and Q4 2013-2018 (intervention group). Primary and secondary outcomes were assessed for confounders and analyzed using both unadjusted and propensity score weighted analyses. Interrupted time-series analyses also analyzed key outcomes.
Results: A total of 3282 and 5456 patients were included in the historical and intervention groups, respectively. There were significant reductions in median antimicrobial duration (5 vs 4 days; P < .001), antimicrobial days of therapy (8 vs 7; P < .001), antimicrobial cost ($96 vs $85; P = .003), length of stay (LOS) (6 vs 5 days; P < .001), intensive care unit (ICU) LOS (3 vs 2 days; P < .001), total hospital cost ($10 946 vs $9119; P < .001), healthcare facility-onset vancomycin-resistant Enterococcus (HO-VRE) incidence (1.3% vs 0.3%; P ≤ .001), and HO-VRE infections (0.6% vs 0.2%; P = .018) in the intervention cohort.
Conclusions: Reductions in antimicrobial use, hospital and ICU LOS, HO-VRE, HO-VRE infections, and costs were associated with incorporation of a novel mortality prediction rule to guide ASP surveillance and intervention.
Keywords: antimicrobial stewardship; assessment tool; mortality risk score.
© The Author(s) 2021. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- Centers for Disease Control and Prevention. Core elements of hospital antibiotic stewardship programs. Available at: https://www.cdc.gov/antibiotic-use/core-elements/index.html. Accessed 6 July 2020. - PMC - PubMed
-
- Alshakrah MA, Steinke DT, Lewis PJ. Patient prioritization for pharmaceutical care in hospital: a systematic review of assessment tools. Res Social Adm Pharm 2019; 15:767–79. - PubMed
-
- Kullar R, Goff DA, Schulz LT, et al. The “epic” challenge of optimizing antimicrobial stewardship: the role of electronic medical records and technology. Clin Infect Dis 2013; 57:1005–13. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
