

Transcatheter aortic valve implantation in a 13-year-old child with end-stage heart failure: a case report
- PMID: 33738418
- PMCID: PMC7954252
- DOI: 10.1093/ehjcr/ytab034
Transcatheter aortic valve implantation in a 13-year-old child with end-stage heart failure: a case report
Abstract
Background: Left ventricular non-compaction cardiomyopathy (LVNC) has been reported in association with almost all types of congenital heart valve disease. The presence of LVNC-related ventricular dysfunction increases the perioperative risk in these patients. The advantages of transcatheter treatment modalities outweigh those of surgical strategies, as they avoid cardioplegic arrest and myocardial trauma. To our knowledge, there have been no reports on transcatheter treatment of pure aortic regurgitation in patients with a bicuspid aortic valve (BAV) and concomitant LVNC.
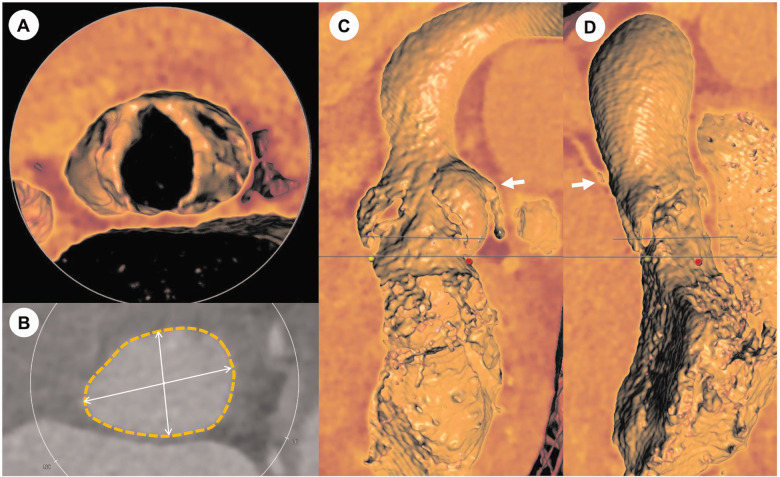
Case summary: In this article, we present the case of a 13-year-old boy with a regurgitant BAV and concomitant LVNC who presented with end-stage heart failure and severe pulmonary hypertension. As a bridge to definitive therapy, the patient underwent an uneventful transcatheter aortic valve implantation (TAVI) using a 26-mm balloon-expandable prosthesis. Device success without paravalvular regurgitation was achieved. At 17 months of follow-up, a steady reduction in pulmonary arterial pressure, persistent normalization of systolic left ventricular function and a tremendous improvement in the patient's physical resilience was observed. The initially considered heart-lung transplantation was avoided and will not be necessary.
Discussion: To the best of our knowledge, this is the first case performed with TAVI for BAV regurgitation in the context of LVNC. With technical modifications and appropriate planning, TAVI in paediatric patients with a non-calcified BAV is feasible. Different imaging modalities revealed an intriguing relationship between aortic regurgitation and morphological signs of a left ventricular non-compaction myocardium.
Keywords: Aortic regurgitation; Bicuspid aortic valve; Case report; End-stage heart failure; Heart transplantation; Left ventricular non-compaction cardiomyopathy; Transcatheter aortic valve implantation or replacement.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures




References
-
- Towbin JA, Lorts A, Jefferies JL.. Left ventricular non-compaction cardiomyopathy. Lancet 2015;386:813–825. - PubMed
-
- Agarwal A, Khandheria BK, Paterick TE, Treiber SC, Bush M, Tajik AJ.. Left ventricular noncompaction in patients with bicuspid aortic valve. J Am Soc Echocardiogr 2013;26:1306–1313. - PubMed
-
- Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ. et al. ; ESC Scientific Document Group. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J 2017;38:2739–2791. - PubMed
-
- Yoon SH, Bleiziffer S, De Backer O, Delgado V, Arai T, Ziegelmueller J. et al. Outcomes in transcatheter aortic valve replacement for bicuspid versus tricuspid aortic valve stenosis. J Am Coll Cardiol 2017;69:2579–2589. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials