

Intraoperative [18F]FDG flexible autoradiography for tumour margin assessment in breast-conserving surgery: a first-in-human multicentre feasibility study
- PMID: 33738563
- PMCID: PMC7973336
- DOI: 10.1186/s13550-021-00759-w
Intraoperative [18F]FDG flexible autoradiography for tumour margin assessment in breast-conserving surgery: a first-in-human multicentre feasibility study
Abstract
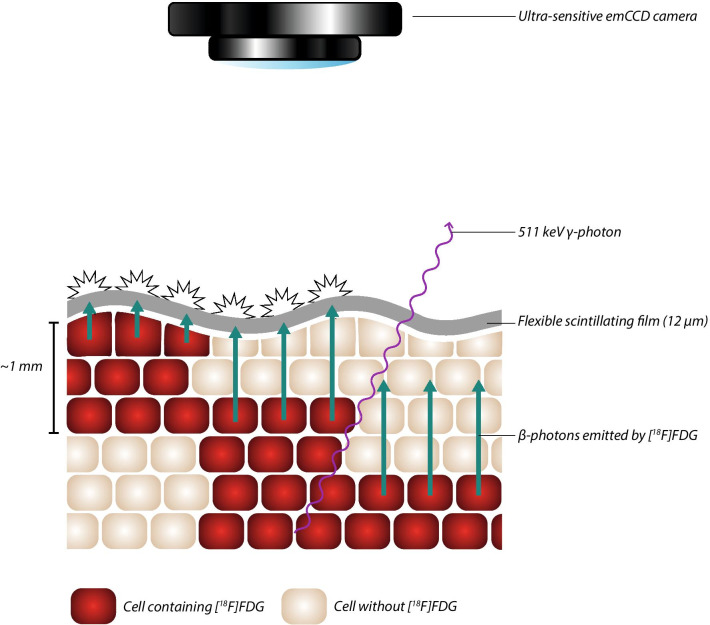
Introduction: In women undergoing breast-conserving surgery (BCS), 20-25% require a re-operation as a result of incomplete tumour resection. An intra-operative technique to assess tumour margins accurately would be a major advantage. A novel method for intraoperative margin assessment was developed by applying a thin flexible scintillating film to specimens-flexible autoradiography (FAR) imaging. A single-arm, multi-centre study was conducted to evaluate the feasibility of intraoperative [18F]FDG FAR for the assessment of tumour margins in BCS.
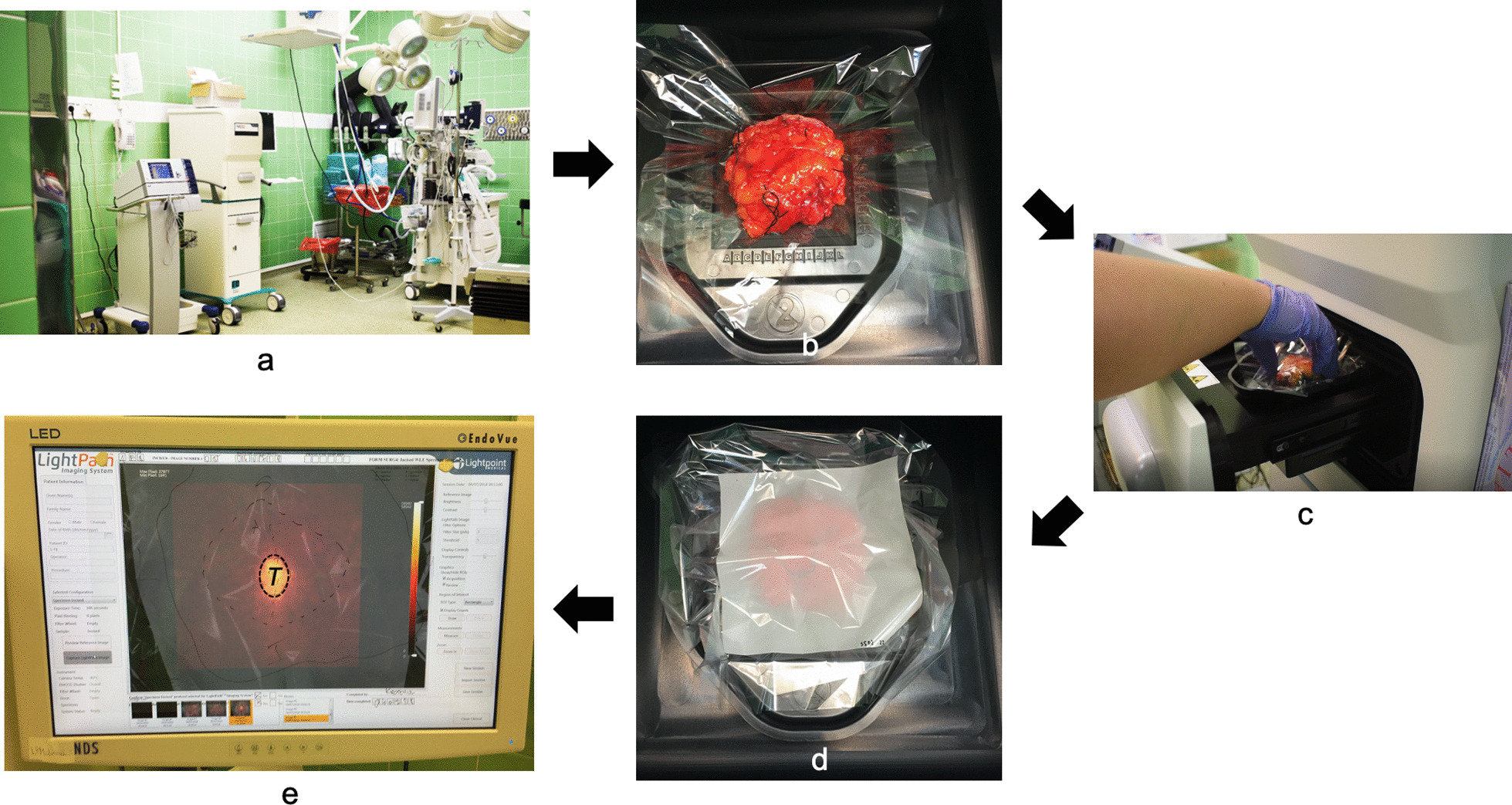
Methods: Eighty-eight patients with invasive breast cancer undergoing BCS received ≤ 300 MBq of [18F]FDG 60-180 min pre-operatively. Following surgical excision, intraoperative FAR imaging was performed using the LightPath® Imaging System. The first 16 patients were familiarisation patients; the remaining 72 patients were entered into the main study. FAR images were analysed post-operatively by three independent readers. Areas of increased signal intensity were marked, mean normalised radiances and tumour-to-tissue background (TBR) determined, agreement between histopathological margin status and FAR assessed and radiation dose to operating theatre staff measured. Subgroup analyses were performed for various covariates, with thresholds set based on ROC curves.
Results: Data analysis was performed on 66 patients. Intraoperative margin assessment using FAR was completed on 385 margins with 46.2% sensitivity, 81.7% specificity, 8.1% PPV, 97.7% NPV and an overall accuracy of 80.5%, detecting both invasive carcinoma and DCIS. A subgroup analysis based on [18F]FDG activity present at time of imaging revealed an increased sensitivity (71.4%), PPV (9.3%) and NPV (98.4%) in the high-activity cohort with mean tumour radiance and TBR of 126.7 ± 45.7 photons/s/cm2/sr/MBq and 2.1 ± 0.5, respectively. Staff radiation exposure was low (38.2 ± 38.1 µSv).
Conclusion: [18F]FDG FAR is a feasible and safe technique for intraoperative tumour margin assessment. Further improvements in diagnostic performance require optimising the method for scintillator positioning and/or the use of targeted radiopharmaceuticals.
Trial registration: Identifier: NCT02666079. Date of registration: 28 January 2016. URL: https://clinicaltrials.gov/ct2/show/NCT02666079 . ISRCTN registry: Reference: ISRCTN17778965. Date of registration: 11 February 2016. URL: http://www.isrctn.com/ISRCTN17778965 .
Keywords: Breast cancer; Breast-conserving surgery; Flexible autoradiography; Margin assessment; Re-operation rate.
Conflict of interest statement
Professor Arnie Purushotham is joint chief investigator for the Experimental Cancer Medicine Centre which is jointly funded by Cancer Research UK and the National Institute for Health Research. Maarten R. Grootendorst and Kunal N. Vyas are both employees of and shareholders in Lightpoint Medical Ltd. There are no other relevant potential conflicts of interest to declare.
Figures


References
-
- Pleijhuis RG, Graafland M, De Vries J, Bart J, De Jong JS, Van Dam GM. Obtaining adequate surgical margins in breast-conserving therapy for patients with early-stage breast cancer: current modalities and future directions. Ann Surg Oncol. 2009;16:2717–2730. doi: 10.1245/s10434-009-0609-z. - DOI - PMC - PubMed
-
- Talsma AK, Reedijk AMJ, Damhuis RAM, Westenend PJ, Vles WJ. Re-resection rates after breast-conserving surgery as a performance indicator: introduction of a case-mix model to allow comparison between Dutch hospitals. Eur J Surg Oncol J Eur Soc Surg Oncol Br Assoc Surg Oncol. 2011;37:357–363. - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
