

Incidental findings in and around the prostate on prostate MRI: a pictorial review
- PMID: 33738590
- PMCID: PMC7973355
- DOI: 10.1186/s13244-021-00979-7
Incidental findings in and around the prostate on prostate MRI: a pictorial review
Abstract
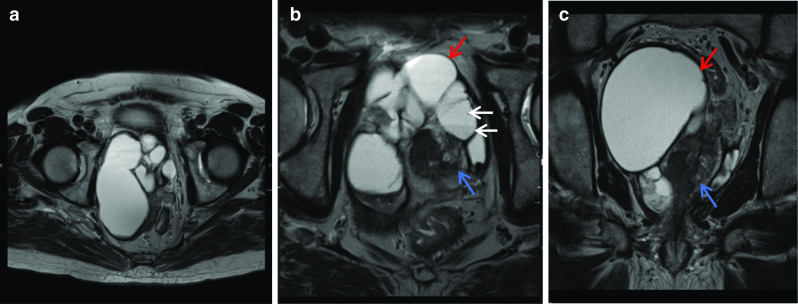
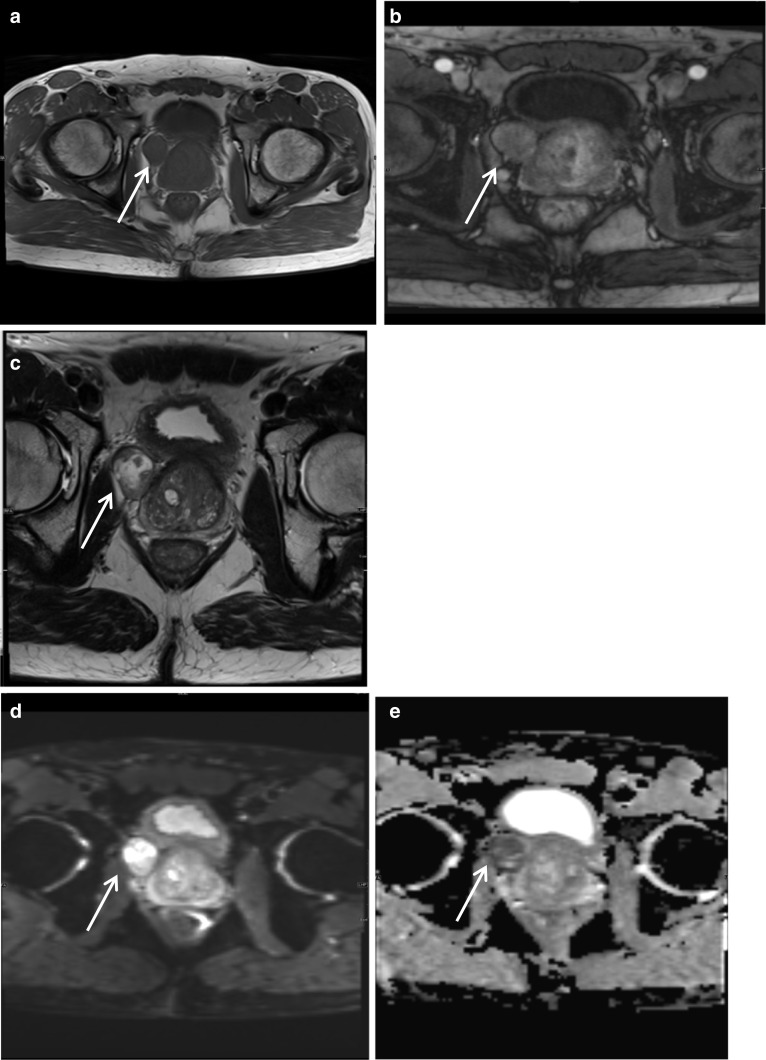
Prostate MRI has seen rapid growth in use in recent years as an advanced diagnostic modality to detect focal areas of clinically significant prostate cancer, to identify an area for targeted biopsy and to guide management and surveillance. The increase in use has also led to increased diagnosis of incidental lesions arising from structures around the prostate. These incidental findings may be related to the genitourinary system or non- genitourinary system and may have a benign aetiology which needs no additional follow-up, or it may require surveillance and management. The field of view in a multiparametric prostate MRI includes other pelvic organs, neurovascular bundles, bowel, lymph nodes and bones. Being familiar with standard MRI characteristics and a sound knowledge of anatomy of the prostate and surrounding structures can help in distinguishing normal anatomy from pathology. Given that patients undertaking a prostate MRI are usually a cohort with increased anxiety from their known or suspicion of prostate cancer, it is important that radiologists are familiar with these common incidental findings to minimise anxiety to the patient, have a well-informed discussion with the referring clinician and reduce costs associated with unnecessary further testing and follow-up of benign incidental findings. Additionally, being able to diagnose more serious incidental pathologies early can be life-saving and potentially significantly alter patient management.
Keywords: Findings; Incidental; MpMRI; Periprostatic.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




















References
-
- American College of Radiology. Prostate Imaging—Reporting and Data System. 2019. Version 2.1. PI-RADS
-
- Shin T, Smyth TB, Ukimura O, et al. Diagnostic accuracy of a five-point Likert scoring system for magnetic resonance imaging (MRI) evaluated according to results of MRI/ultrasonography image-fusion targeted biopsy of the prostate. BJU Int. 2018;121:77–83. doi: 10.1111/bju.13972. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
