

Posterior uveal melanoma incidence and survival by AJCC tumour size in a 70-year nationwide cohort
- PMID: 33738986
- PMCID: PMC9543793
- DOI: 10.1111/aos.14847
Posterior uveal melanoma incidence and survival by AJCC tumour size in a 70-year nationwide cohort
Abstract
Purpose: While early treatment of posterior uveal melanoma can save the eye, the effect of early treatment on survival remains unknown. Therefore, we aimed to determine whether the tumour size at diagnosis has changed over time, and if this has affected survival rates of patients with posterior uveal melanoma in Denmark.
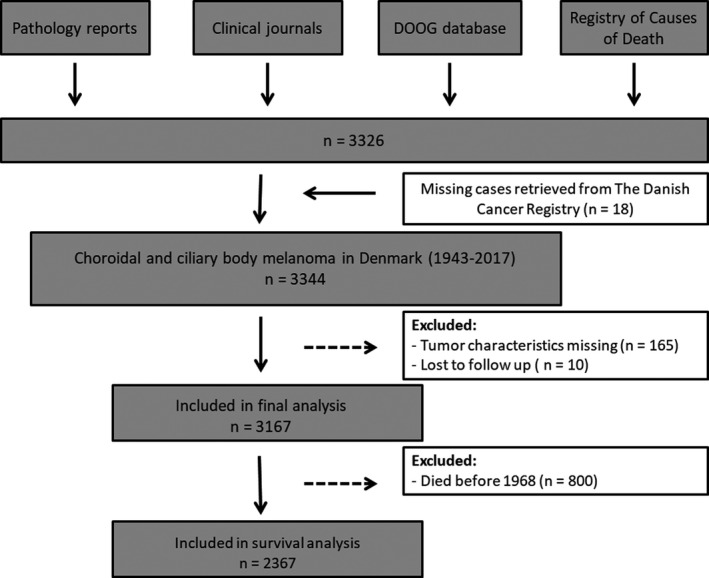
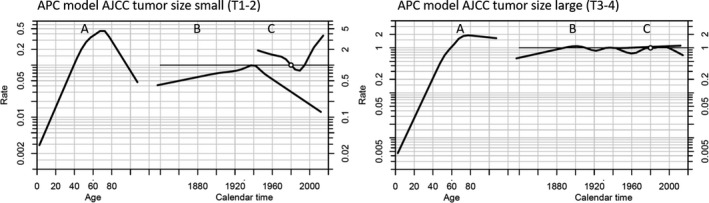
Methods: Nationwide retrospective cohort study linking data from registry-based resources to data from clinical charts and pathology records. Including all Danish patients diagnosed with posterior uveal melanoma from 1943 to 2017. Incidence rates were estimated as annual percentage change (APC) overall and by American Joint Committee on Cancer (AJCC) tumour sizes. The age-period-cohort model was applied to estimate the relative risk of calendar period. The cox proportional hazards model, relative survival Kaplan-Meier curves and cumulative incidence curves were applied to estimate the effect of calendar period on survival.
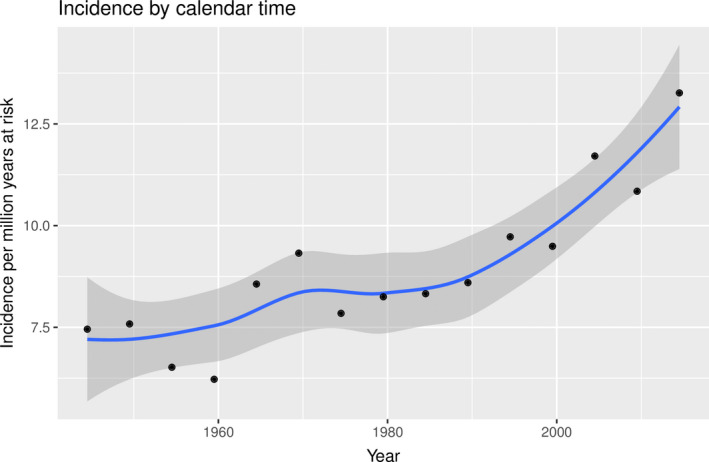
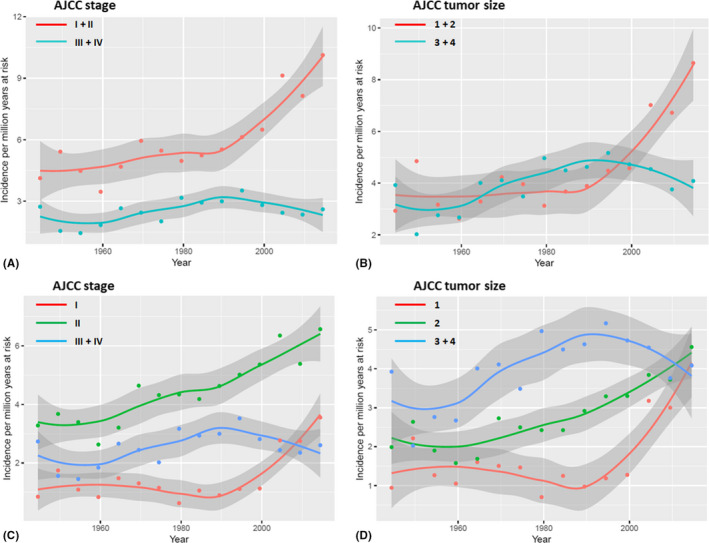
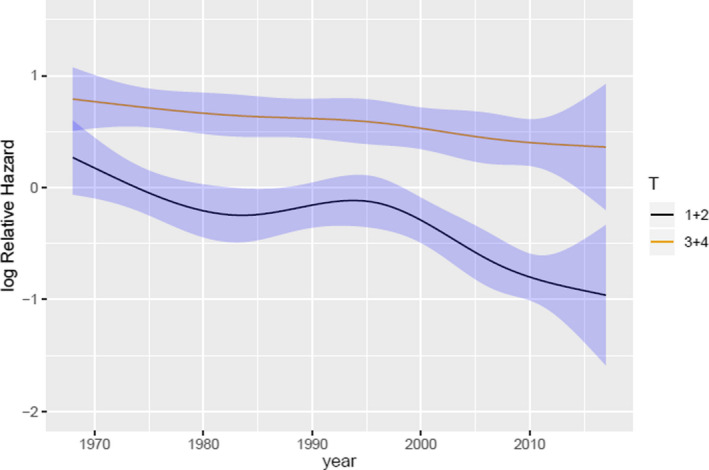
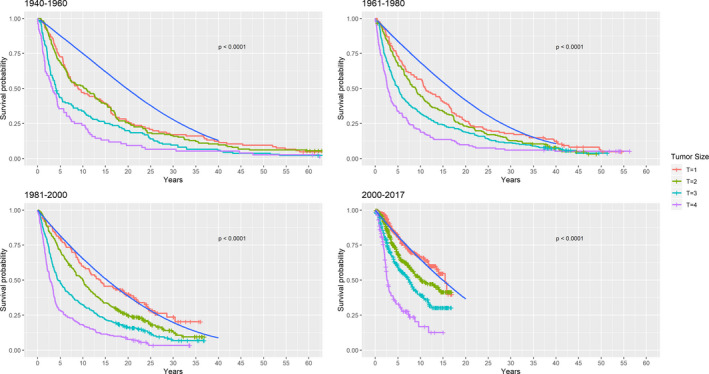
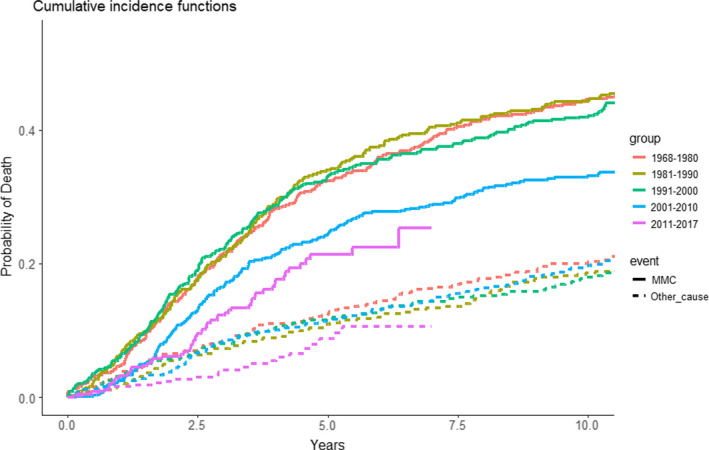
Results: An overall increase in incidence rate of uveal melanoma was found (APC = 0.25%, 0.08-0.42; 95% CI). This was due to increasing incidence rate of AJCC T1 + T2 tumours (APC = 0.97%, 0.57-1.37; 95% CI), whereas no increase in incidence rates of AJCC T3 + T4 tumours was found (APC = -0.01%, -0.26 to 0.25; 95% CI). The disease-specific survival improved with calendar period for all tumour sizes (HR = 0.988; 0.984-0.993; 95% CI).
Conclusion: Increasing incidence rate and improved survival rate for uveal melanoma was found concordantly with a decrease in tumour size during a 70-year period.
© 2021 The Authors. Acta Ophthalmologica published by John Wiley & Sons Ltd on behalf of Acta Ophthalmologica Scandinavica Foundation.
Figures
References
-
- Ah‐Fat F & Damato B (1998): Delays in the diagnosis of uveal melanoma and effect on treatment. Eye 12: 781–782. - PubMed
-
- Andersson TML, Rutherford MJ & Humphreys K (2017): Assessment of lead‐time bias in estimates of relative survival for breast cancer. Cancer Epidemiol 46: 50–56. - PubMed
-
- Bagger M, Andersen MT, Andersen KK, Heegaard S, Andersen MK & Kiilgaard JF (2014): The prognostic effect of American Joint Committee on Cancer staging and genetic status in patients with choroidal and ciliary body melanoma. Invest Ophthalmol Vis Sci 56: 438–444. - PubMed
-
- Bagger M, Smidt‐Nielsen I, Andersen MK, Jensen PK, Heegaard S, Andersen KK, Friis S & Kiilgaard JF (2018): Long‐term metastatic risk after biopsy of posterior uveal melanoma. Ophthalmology 1–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
