

Reduced-iodine-dose dual-energy coronary CT angiography: qualitative and quantitative comparison between virtual monochromatic and polychromatic CT images
- PMID: 33740093
- PMCID: PMC8379124
- DOI: 10.1007/s00330-021-07809-w
Reduced-iodine-dose dual-energy coronary CT angiography: qualitative and quantitative comparison between virtual monochromatic and polychromatic CT images
Abstract
Objectives: To quantitatively evaluate the impact of virtual monochromatic images (VMI) on reduced-iodine-dose dual-energy coronary computed tomography angiography (CCTA) in terms of coronary lumen segmentation in vitro, and secondly to assess the image quality in vivo, compared with conventional CT obtained with regular iodine dose.
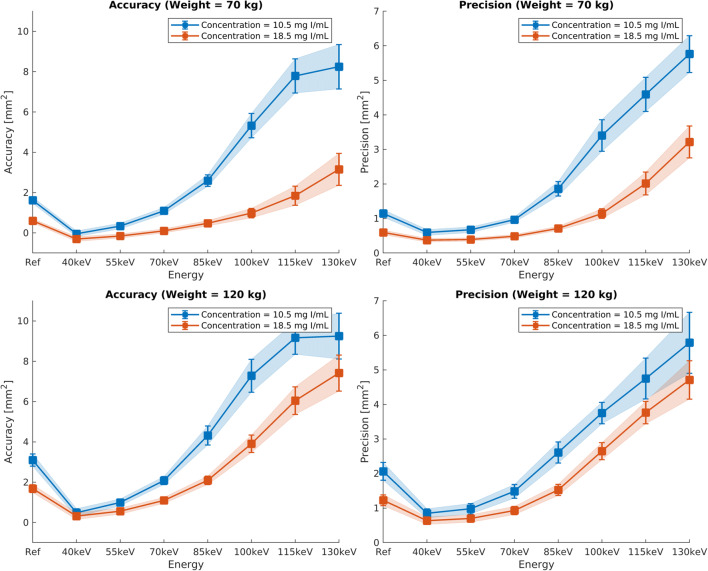
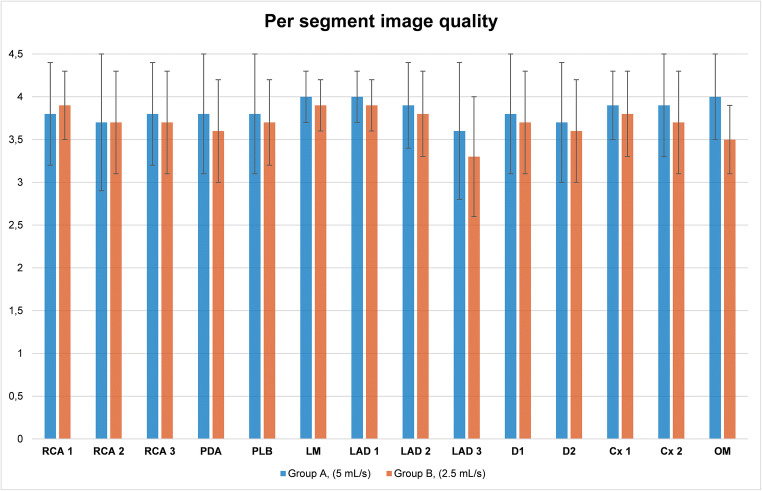
Materials and methods: A phantom simulating regular and reduced iodine injection was used to determine the accuracy and precision of lumen area segmentation for various VMI energy levels. We retrospectively included 203 patients from December 2017 to August 2018 (mean age, 51.7 ± 16.8 years) who underwent CCTA using either standard (group A, n = 103) or reduced (group B, n = 100) iodine doses. Conventional images (group A) were qualitatively and quantitatively compared with 55-keV VMI (group B). We recorded the location of venous catheters.
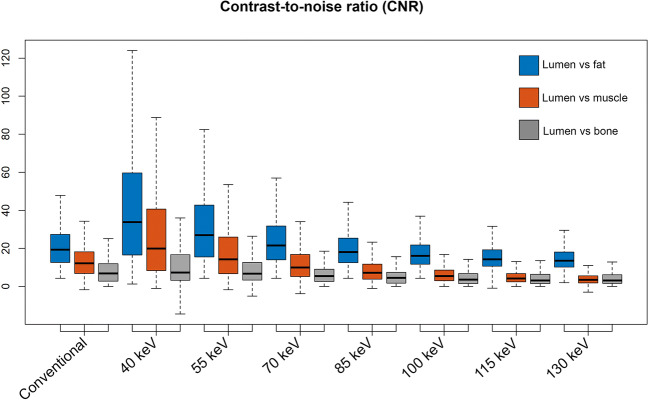
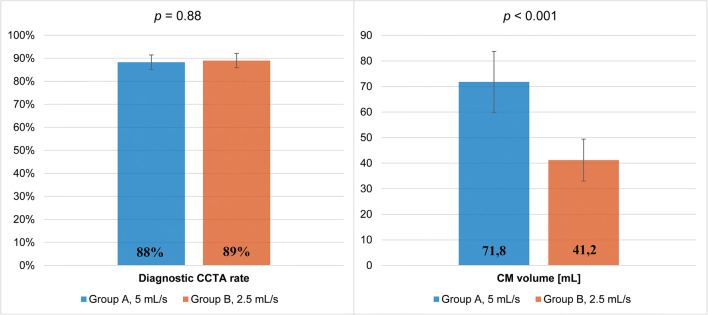
Results: In vitro, VMI outperformed conventional CT, with a segmentation accuracy of 0.998 vs. 1.684 mm2, respectively (p < 0.001), and a precision of 0.982 vs. 1.229 mm2, respectively (p < 0.001), in simulated overweight adult subjects. In vivo, the rate of diagnostic CCTA in groups A and B was 88.4% (n = 91/103) vs. 89% (n = 89/100), respectively, and noninferiority of protocol B was inferred. Contrast-to-noise ratios (CNR) of lumen versus fat and muscle were higher in group B (p < 0.001) and comparable for lumen versus calcium (p = 0.423). Venous catheters were more often placed on the forearm or hand in group B (p < 0.001).
Conclusion: In vitro, low-keV VMI improve vessel area segmentation. In vivo, low-keV VMI allows for a 40% iodine dose and injection rate reduction while maintaining diagnostic image quality and improves the CNR between lumen versus fat and muscle.
Key points: • Dual-energy coronary CT angiography is becoming increasingly available and might help improve patient management. • Compared with regular-iodine-dose coronary CT angiography, reduced-iodine-dose dual-energy CT with low-keV monochromatic image reconstructions performed better in phantom-based vessel cross-sectional segmentation and proved to be noninferior in vivo. • Patients receiving reduced-iodine-dose dual-energy coronary CT angiography often had the venous catheter placed on the forearm or wrist without compromising image quality.
Keywords: Computed tomography angiography; Coronary vessels; Dimensional measurement accuracy; Iodine; Phantoms, imaging.
© 2021. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
References
-
- American College of Radiology (2020) ACR manual on contrast media v10.3. Available via https://www.acr.org/-/media/ACR/Files/Clinical-Resources/Contrast_Media.pdf. Accessed Apr 18 2020
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
