

An international survey on aminoglycoside practices in critically ill patients: the AMINO III study
- PMID: 33740157
- PMCID: PMC7979853
- DOI: 10.1186/s13613-021-00834-4
An international survey on aminoglycoside practices in critically ill patients: the AMINO III study
Abstract
Background: While aminoglycosides (AG) have been used for decades, debate remains on their optimal dosing strategy. We investigated the international practices of AG usage specifically regarding dosing and therapeutic drug monitoring (TDM) in critically ill patients. We conducted a prospective, multicentre, observational, cohort study in 59 intensive-care units (ICUs) in 5 countries enrolling all ICU patients receiving AG therapy for septic shock.
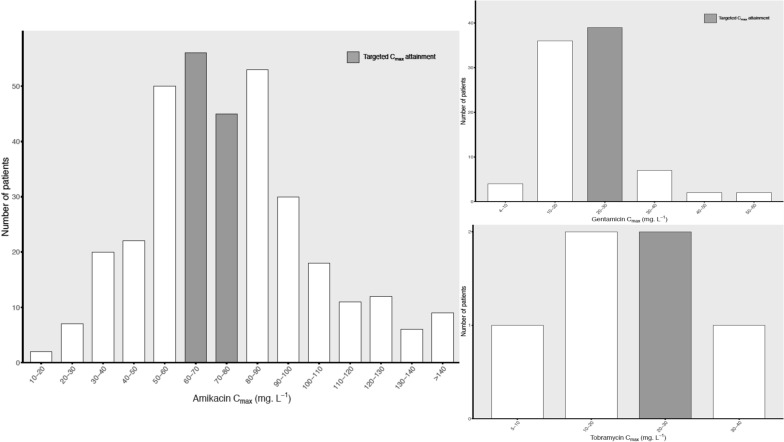
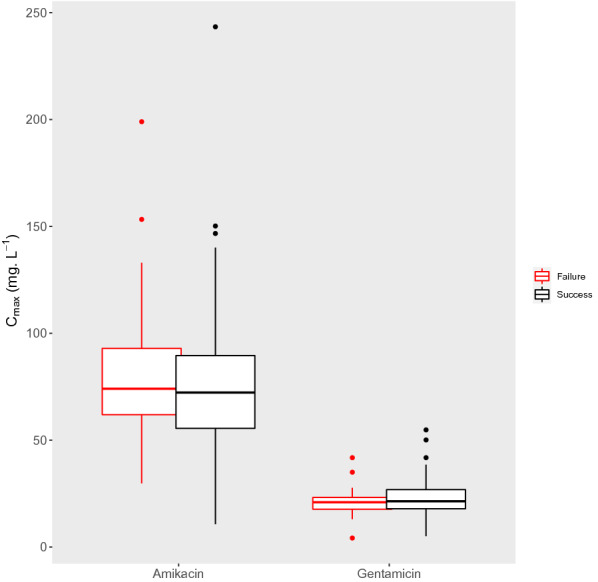
Results: We enrolled 931 septic ICU patients [mean ± standard deviation, age 63 ± 15 years, female 364 (39%), median (IQR) SAPS II 51 (38-65)] receiving AG as part of empirical (761, 84%) or directed (147, 16%) therapy. The AG used was amikacin in 614 (66%), gentamicin in 303 (33%), and tobramycin in 14 (1%) patients. The median (IQR) duration of therapy was 2 (1-3) days, the number of doses was 2 (1-2), the median dose was 25 ± 6, 6 ± 2, and 6 ± 2 mg/kg for amikacin, gentamicin, and tobramycin respectively, and the median dosing interval was 26 (23.5-43.5) h. TDM of Cmax and Cmin was performed in 437 (47%) and 501 (57%) patients, respectively, after the first dose with 295 (68%) patients achieving a Cmax/MIC > 8 and 353 (71%) having concentrations above Cmin recommended thresholds. The ICU mortality rate was 27% with multivariable analysis showing no correlation between AG dosing or pharmacokinetic/pharmacodynamic target attainment and clinical outcomes.
Conclusion: Short courses of high AG doses are mainly used in ICU patients with septic shock, although wide variability in AG usage is reported. We could show no correlation between PK/PD target attainment and clinical outcome. Efforts to optimize the first AG dose remain necessary. Trial registration Clinical Trials, NCT02850029, registered on 29th July 2016, retrospectively registered, https://www.clinicaltrials.gov.
Keywords: Aminoglycoside; Antibiotics; ICU; PK/PD; Therapeutic drug monitoring.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, Suppes R, Feinstein D, Zanotti S, Taiberg L, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34(6):1589–1596. doi: 10.1097/01.CCM.0000217961.75225.E9. - DOI - PubMed
-
- Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, Sevransky JE, Sprung CL, Douglas IS, Jaeschke R, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580–637. doi: 10.1097/CCM.0b013e31827e83af. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
