

Recommendations for tilt table testing and other provocative cardiovascular autonomic tests in conditions that may cause transient loss of consciousness : Consensus statement of the European Federation of Autonomic Societies (EFAS) endorsed by the American Autonomic Society (AAS) and the European Academy of Neurology (EAN)
- PMID: 33740206
- PMCID: PMC8184725
- DOI: 10.1007/s10286-020-00738-6
Recommendations for tilt table testing and other provocative cardiovascular autonomic tests in conditions that may cause transient loss of consciousness : Consensus statement of the European Federation of Autonomic Societies (EFAS) endorsed by the American Autonomic Society (AAS) and the European Academy of Neurology (EAN)
Abstract
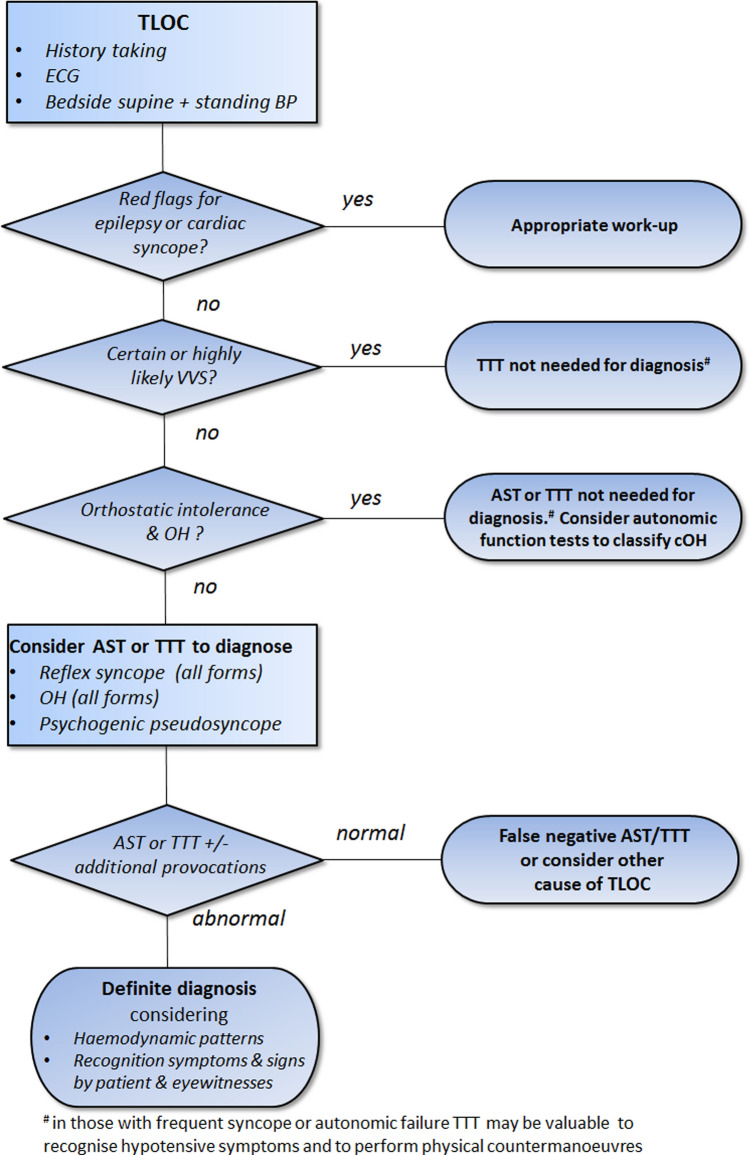
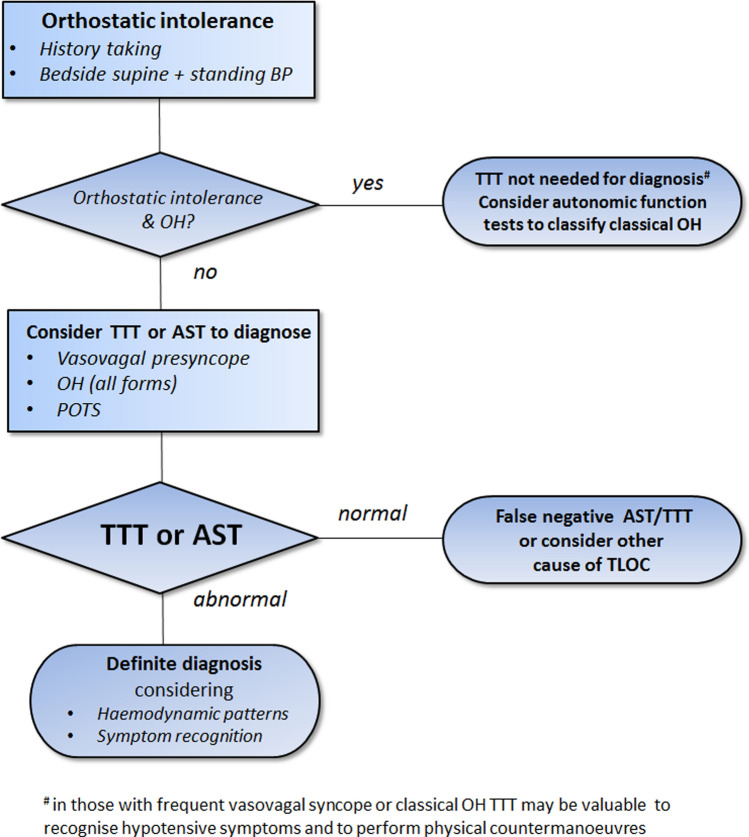
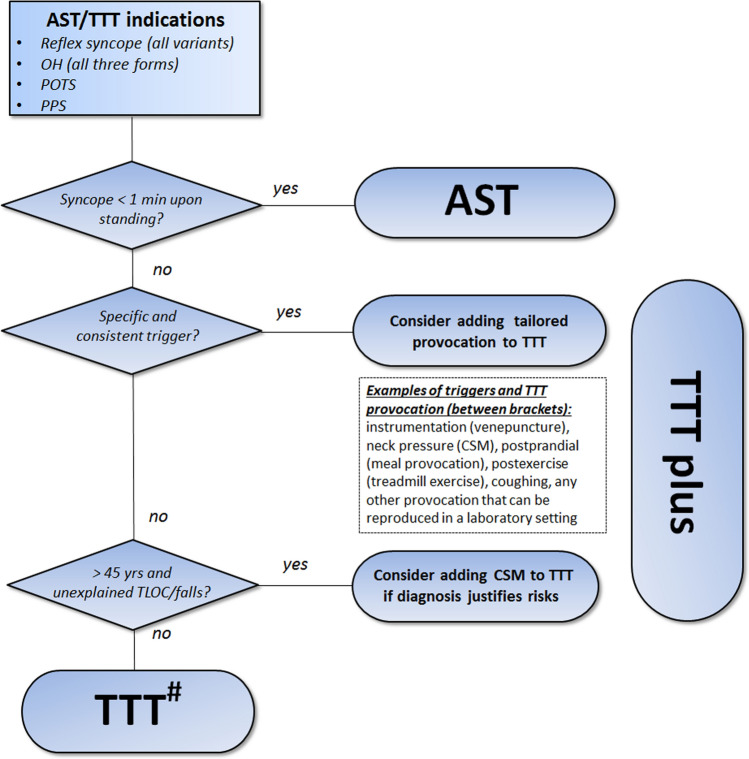
An expert committee was formed to reach consensus on the use of tilt table testing (TTT) in the diagnosis of disorders that may cause transient loss of consciousness (TLOC) and to outline when other provocative cardiovascular autonomic tests are needed. While TTT adds to history taking, it cannot be a substitute for it. An abnormal TTT result is most meaningful if the provoked event is recognised by patients or eyewitnesses as similar to spontaneous events. The minimum requirements to perform TTT are a tilt table, a continuous beat-to-beat blood pressure monitor, at least one ECG lead, protocols for the indications stated below and trained staff. This basic equipment lends itself to the performance of (1) additional provocation tests, such as the active standing test, carotid sinus massage and autonomic function tests; (2) additional measurements, such as video, EEG, transcranial Doppler, NIRS, end-tidal CO2 or neuro-endocrine tests; and (3) tailor-made provocation procedures in those with a specific and consistent trigger of TLOC. TTT and other provocative cardiovascular autonomic tests are indicated if the initial evaluation does not yield a definite or highly likely diagnosis, but raises a suspicion of (1) reflex syncope, (2) the three forms of orthostatic hypotension (OH), i.e. initial, classic and delayed OH, as well as delayed orthostatic blood pressure recovery, (3) postural orthostatic tachycardia syndrome or (4) psychogenic pseudosyncope. A therapeutic indication for TTT is to teach patients with reflex syncope and OH to recognise hypotensive symptoms and to perform physical counter manoeuvres.
Keywords: Orthostatic hypotension; Psychogenic pseudosyncope; Reflex syncope; Syncope; Tilt table testing; Transient loss of consciousness; Vasovagal.
Conflict of interest statement
Dr. Thijs reports personal fees from Medtronic, Union Chimique Belge (UCB), GlaxoSmithKline (GSK), Theravance, Novartis and grants from Dutch National Epilepsy Fund, Christelijke Vereniging voor de Verpleging van Lijders aan Epilepsie, AC Thomson Foundation, Medtronic, The Netherlands Organisation for Health Research and Development (843002707), outside the submitted work. Dr Fanciulli reports royalties from Springer Nature Publishing Group and Thieme Verlag, speaker fees from the Austrian Autonomic Society, Austrian Neurology Society, Austrian Parkinson Society, Ordensklinikum Linz, International Parkinson Disease and Movement Disorders Society and Theravance Biopharma, research grants from the Stichting ParkinsonFond, MSA Coalition and the Österreichischer Austausch Dienst, outside the submitted work. Prof Sutton serves as consultant to Medtronic Inc., is a member of the Speakers Bureau of SJM Abbott Laboratories, and shareholder in Edwards Lifesciences and Boston Scientific Corp., outside of the submitted work. Prof Pavy-Le Traon reports a research grant from the French Ministry of Health outside the submitted work. Prof Jordan served as advisor for Novo-Nordisk, Bayer, received research support from Boston Scientific and Boehringer Ingelheim and is cofounder of Eternygen GmbH, outside the submitted work. Prof. Habek participated as clinical investigator, speaker and/or advisor for Biogen, Sanofi Genzyme, Merck, Bayer, Novartis, Pliva/Teva, Roche, Alvogen, Actelion, Alexion Pharmaceuticals, outside the submitted work. Prof Struhal reports consultancy for Boehringer, Eli Lilly, royalties from Manz-Rechtsverlag, Springer, Oxford University Press, speaker fees from Boehringer, Merz, Medconvent, Donau-Universität Krems, Austrian Society of Neurology, Manz-Rechtsverlag. Prof. Hilz received consulting honoraria from Alnylam and Sanofi-Genzyme, lecturing honoraria and travel support from Bayer HealthCare, Amicus, Sanofi-Genzyme, and research funding from Novartis Pharma and Bayer Health Care.
Figures
References
-
- Kenny RA, Ingram A, Bayliss J, Sutton R. Head-up tilt: a useful test for investigating unexplained syncope. Lancet (London, England) 1986;1:1352–1355. - PubMed
-
- Brignole M, Moya A, de Lange FJ, Deharo JC, Elliott PM, Fanciulli A, Fedorowski A, Furlan R, Kenny RA, Martin A, Probst V, Reed MJ, Rice CP, Sutton R, Ungar A, van Dijk JG (2018) 2018 ESC Guidelines for the diagnosis and management of syncope. Eur Heart J - PubMed
-
- Freeman R, Wieling W, Axelrod FB, Benditt DG, Benarroch E, Biaggioni I, Cheshire WP, Chelimsky T, Cortelli P, Gibbons CH, Goldstein DS, Hainsworth R, Hilz MJ, Jacob G, Kaufmann H, Jordan J, Lipsitz LA, Levine BD, Low PA, Mathias C, Raj SR, Robertson D, Sandroni P, Schatz I, Schondorff R, Stewart JM, van Dijk JG. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin Auton Res. 2011;21:69–72. - PubMed
-
- Wieling W, van Dijk N, de Lange FJ, Olde Nordkamp LR, Thijs RD, van Dijk JG, Linzer M, Sutton R. History taking as a diagnostic test in patients with syncope: developing expertise in syncope. Eur Heart J. 2015;36:277–280. - PubMed
-
- Saal DP, Thijs RD, van Dijk JG. Tilt table testing in neurology and clinical neurophysiology. Clin Neurophysiol. 2016;127:1022–1030. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
