

The Association of Intraoperative driving pressure with postoperative pulmonary complications in open versus closed abdominal surgery patients - a posthoc propensity score-weighted cohort analysis of the LAS VEGAS study
- PMID: 33740885
- PMCID: PMC7977277
- DOI: 10.1186/s12871-021-01268-y
The Association of Intraoperative driving pressure with postoperative pulmonary complications in open versus closed abdominal surgery patients - a posthoc propensity score-weighted cohort analysis of the LAS VEGAS study
Abstract
Background: It is uncertain whether the association of the intraoperative driving pressure (ΔP) with postoperative pulmonary complications (PPCs) depends on the surgical approach during abdominal surgery. Our primary objective was to determine and compare the association of time-weighted average ΔP (ΔPTW) with PPCs. We also tested the association of ΔPTW with intraoperative adverse events.
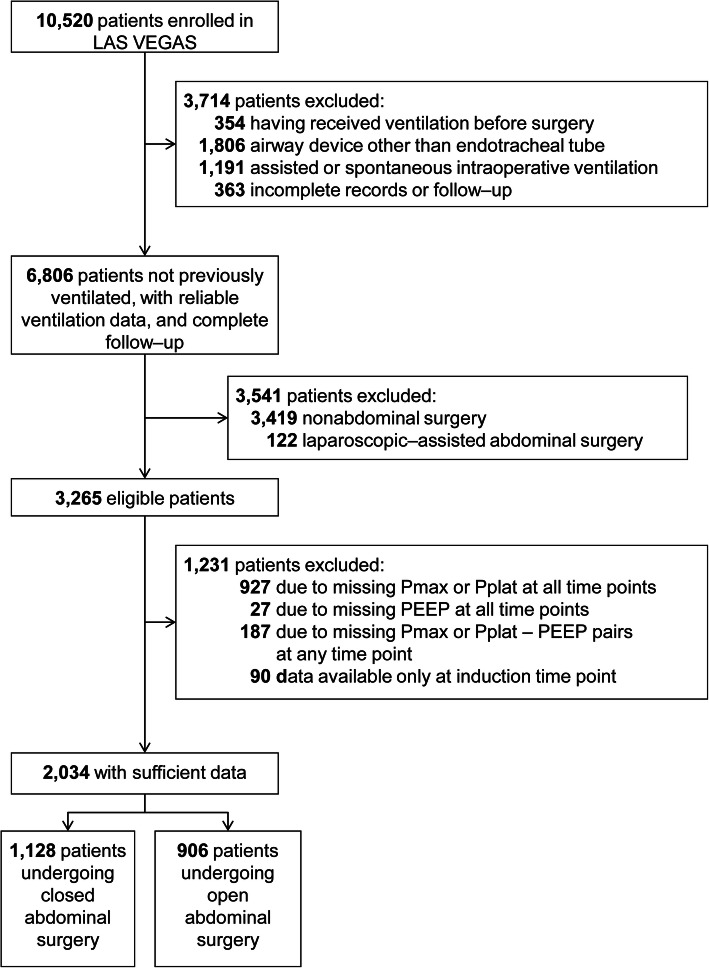
Methods: Posthoc retrospective propensity score-weighted cohort analysis of patients undergoing open or closed abdominal surgery in the 'Local ASsessment of Ventilatory management during General Anaesthesia for Surgery' (LAS VEGAS) study, that included patients in 146 hospitals across 29 countries. The primary endpoint was a composite of PPCs. The secondary endpoint was a composite of intraoperative adverse events.
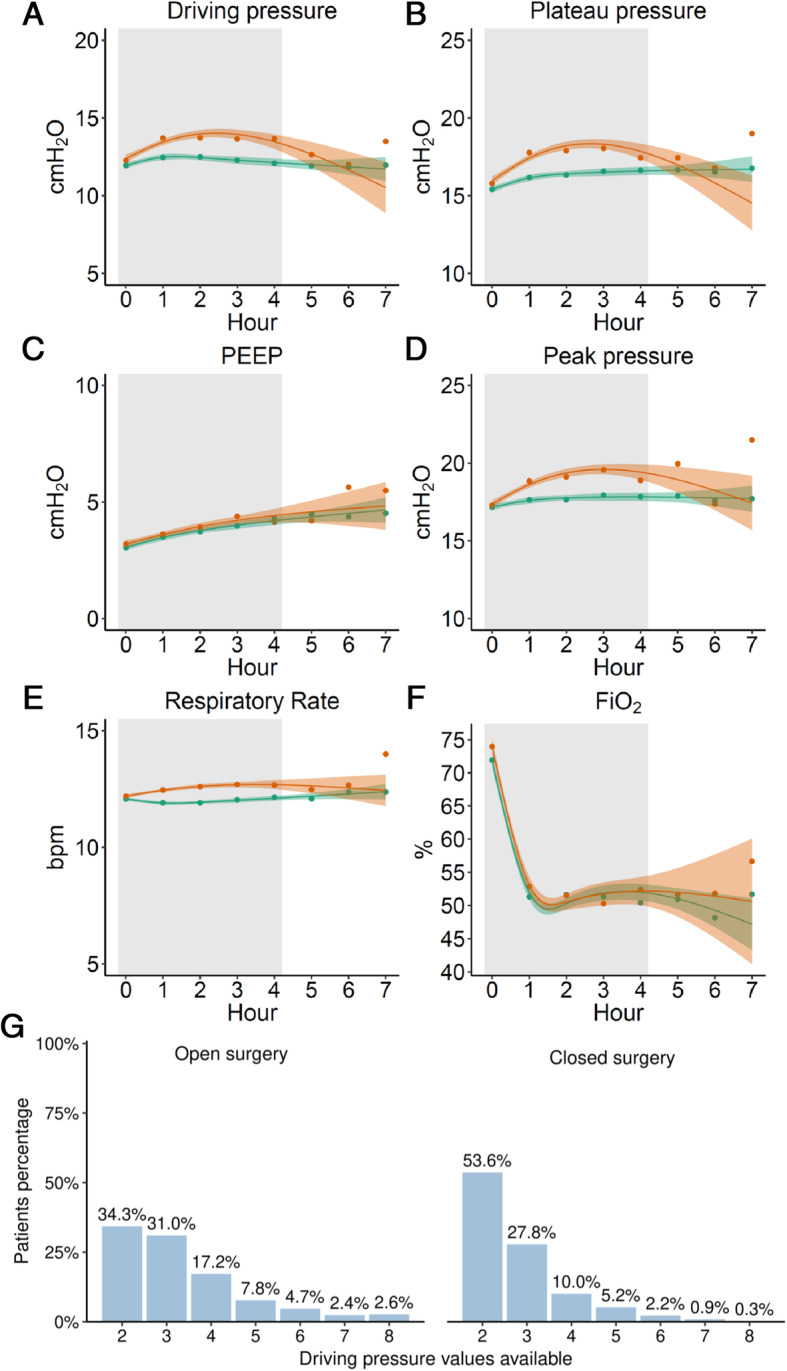
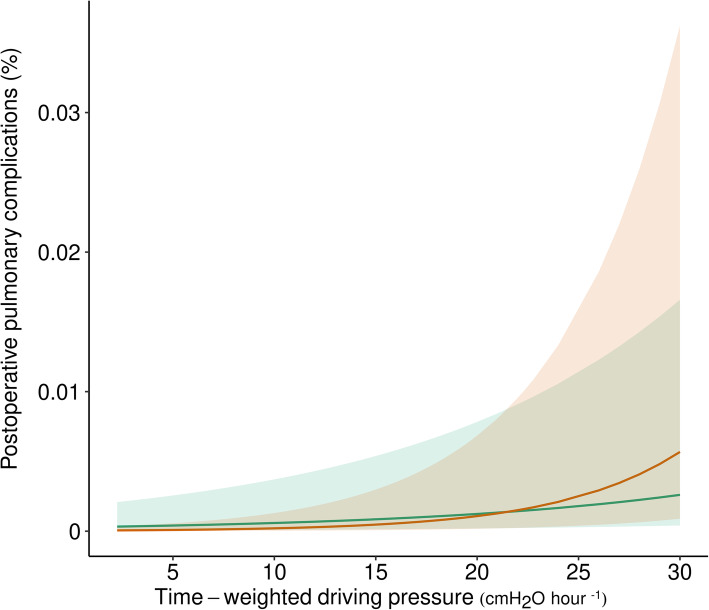
Results: The analysis included 1128 and 906 patients undergoing open or closed abdominal surgery, respectively. The PPC rate was 5%. ΔP was lower in open abdominal surgery patients, but ΔPTW was not different between groups. The association of ΔPTW with PPCs was significant in both groups and had a higher risk ratio in closed compared to open abdominal surgery patients (1.11 [95%CI 1.10 to 1.20], P < 0.001 versus 1.05 [95%CI 1.05 to 1.05], P < 0.001; risk difference 0.05 [95%CI 0.04 to 0.06], P < 0.001). The association of ΔPTW with intraoperative adverse events was also significant in both groups but had higher odds ratio in closed compared to open abdominal surgery patients (1.13 [95%CI 1.12- to 1.14], P < 0.001 versus 1.07 [95%CI 1.05 to 1.10], P < 0.001; risk difference 0.05 [95%CI 0.030.07], P < 0.001).
Conclusions: ΔP is associated with PPC and intraoperative adverse events in abdominal surgery, both in open and closed abdominal surgery.
Trial registration: LAS VEGAS was registered at clinicaltrials.gov (trial identifier NCT01601223 ).
Keywords: Driving pressure; Laparoscopic surgery; Laparoscopy; PEEP; Perioperative ventilation; Pneumoperitoneum; Protective ventilation; Respiratory mechanics.
Conflict of interest statement
G. Mazzinari: No interest declared; A. Serpa Neto: No interest declared; S.N.T. Hemmes: No interest declared; G. Hedenstierna: No interest declared; S. Jaber: No interest declared; M. Hiesmayr: No interest declared; M.W. Hollmann: Executive Section Editor Pharmacology with Anesthesia & Analgesia, Section Editor Anesthesiology with Journal of Clinical Medicine, and CSL Behring, no conflict of interest with the current work; G.H. Mills: No interest declared; M.F. Vidal Melo: is funded by NIH/NHLBI grant UH3-HL140177; R.M. Pearse: No interest declared; C. Putensen: No interest declared; W. Schmid: No interest declared; P. Severgnini: No interest declared; H.Wrigge: No interest declared; O. Diaz–Cambronero: had received a Merck Sharp & Dohme investigator–initiated grant (protocol code #53607). Sponsors and funders have no roles in study design, analysis of data or reporting. Also received speakers fees for lecture and medical advice from Merck Sharp & Dohme, no conflict of interest with the current work; L.Ball: No interest declared; M. Gama de Abreu: Ambu, GE Healthcare, ZOLL consulting fees, no conflict of interest with the current work; P.Pelosi: No interest declared; M.J.Schultz: No interest declared.
Figures
References
-
- Neto AS, Hemmes SNT, Barbas CSV, et al. Association between driving pressure and development of postoperative pulmonary complications in patients undergoing mechanical ventilation for general anaesthesia: a meta-analysis of individual patient data. Lancet Respir Med. 2016;4:272–280. doi: 10.1016/S2213-2600(16)00057-6. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
