

Characterization of self-anticipated pain score prior to elective surgery - a prospective observational study
- PMID: 33740887
- PMCID: PMC7977573
- DOI: 10.1186/s12871-021-01303-y
Characterization of self-anticipated pain score prior to elective surgery - a prospective observational study
Abstract
Background: Current principles of postoperative pain management are primarily based on the types and extent of surgical intervention. This clinical study measured patient's self-anticipated pain score before surgery, and compared the anticipated scores with the actual pain levels and analgesic requirements after surgery.
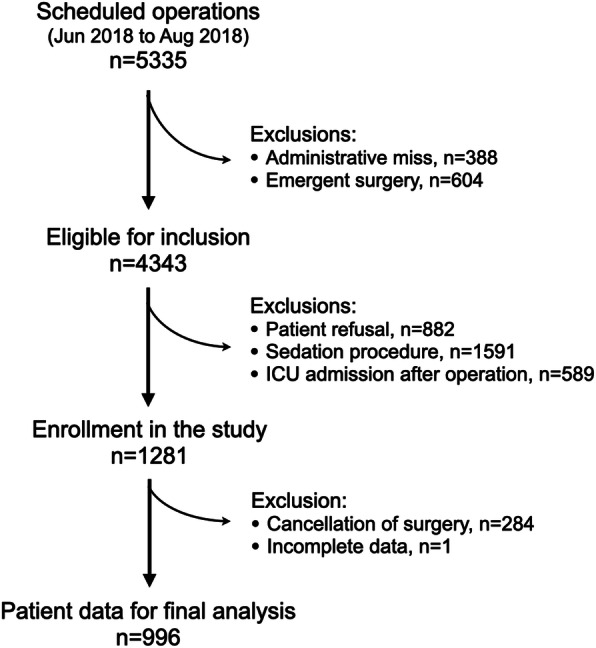
Methods: This prospective observational study recruited consecutive patients who received elective surgery in the E-Da Hospital, Taiwan from June to August 2018. Patients were asked to subjectively rate their highest anticipated pain level (numeric rating scale, NRS 0-10) for the scheduled surgical interventions during their preoperative anesthesia assessment. After the operation, the actual pain intensity (NRS 0-10) experienced by the patient in the post-anesthesia care unit and the total dose of opioids administered during the perioperative period were recorded. Pain scores ≥4 on NRS were regarded as being unacceptable levels for anticipated or postoperative pain that required more aggressive intervention.
Results: A total of 996 patients were included in the study. Most of the patients (86%) received general anesthesia and 73.9% of them had a history of previous operation. Female anticipated significantly higher overall pain intensities than the male patients (adjusted odd ratio 1.523, 95% confidence interval 1.126-2.061; P = 0.006). Patients who took regular benzodiazepine at bedtime (P = 0.037) and those scheduled to receive more invasive surgical procedures were most likely to anticipate for higher pain intensity at the preoperative period (P < 0.05). Higher anticipated pain scores (preoperative NRS ≥ 4) were associated with higher actual postoperative pain levels (P = 0.007) in the PACU and higher total equivalent opioid use (P < 0.001) for acute pain management during the perioperative period.
Conclusion: This observational study found that patients who are female, use regular benzodiazepines at bedtime and scheduled for more invasive surgeries anticipate significantly higher surgery-related pain. Therefore, appropriate preoperative counseling for analgesic control and the management of exaggerated pain expectation in these patients is necessary to improve the quality of anesthesia delivered and patient's satisfaction.
Keywords: Numeric rating scale; Pain expectation; Pre-anesthesia assessment, post-anesthesia care unit; Surgery-related pain.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


Similar articles
-
[Oral therapy algorithm for the treatment of postoperative pain. A prospective observational study].Schmerz. 2013 Feb;27(1):26-37. doi: 10.1007/s00482-012-1279-5. Schmerz. 2013. PMID: 23321702 German.
-
Perioperative pregabalin for reducing pain, analgesic consumption, and anxiety and enhancing sleep quality in elective neurosurgical patients: a prospective, randomized, double-blind, and controlled clinical study.J Neurosurg. 2016 Dec;125(6):1513-1522. doi: 10.3171/2015.10.JNS151516. Epub 2016 Feb 12. J Neurosurg. 2016. PMID: 26871201 Clinical Trial.
-
Pain in neurosurgically treated patients: a prospective observational study.J Neurosurg. 2006 Mar;104(3):350-9. doi: 10.3171/jns.2006.104.3.350. J Neurosurg. 2006. PMID: 16572646
-
Prevalence of pain 6 months after surgery: a prospective observational study.BMC Anesthesiol. 2016 Oct 10;16(1):91. doi: 10.1186/s12871-016-0261-7. BMC Anesthesiol. 2016. PMID: 27724844 Free PMC article.
-
Preoperative anxiety.Curr Opin Anaesthesiol. 2022 Dec 1;35(6):674-678. doi: 10.1097/ACO.0000000000001186. Epub 2022 Sep 21. Curr Opin Anaesthesiol. 2022. PMID: 36131642 Review.
Cited by
-
Investigating Factors Associated with the Development of Postnatal Depression After Cesarean Delivery: A Validation Cohort Study.Neuropsychiatr Dis Treat. 2024 Feb 29;20:439-447. doi: 10.2147/NDT.S448853. eCollection 2024. Neuropsychiatr Dis Treat. 2024. PMID: 38439945 Free PMC article.
-
Surgery patients' perspectives of their role in postoperative pain: A scoping review.Int J Nurs Stud Adv. 2023 Mar 30;5:100124. doi: 10.1016/j.ijnsa.2023.100124. eCollection 2023 Dec. Int J Nurs Stud Adv. 2023. PMID: 38746556 Free PMC article.
-
Cutoff Values for Providing the Ideal Intravenous Patient-Controlled Analgesia According to the Intensity of Postoperative Pain-A Retrospective Observational Study.Medicina (Kaunas). 2021 Oct 6;57(10):1065. doi: 10.3390/medicina57101065. Medicina (Kaunas). 2021. PMID: 34684102 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
